Visual prognosis of vitrectomy for polypoidal choroidal vasculopathy with breakthrough vitreous hemorrhage
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
摘要
Aim: The objective of this study was to investigate the prognosis of massive vitreous hemorrhage (VH) secondary to polypoidal choroidal vasculopathy (PCV) after vitrectomy.
Methods: Forty-nine eyes in 48 patients with PCV and breakthrough VH who underwent 23-gauge pars plana vitrectomy (PPV) between January 2015 and December 2020 were enrolled. The main outcome parameters were best-corrected visual acuity, postoperative adverse events, and reoperation.
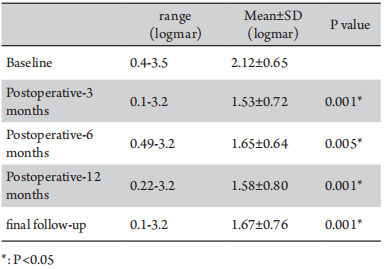
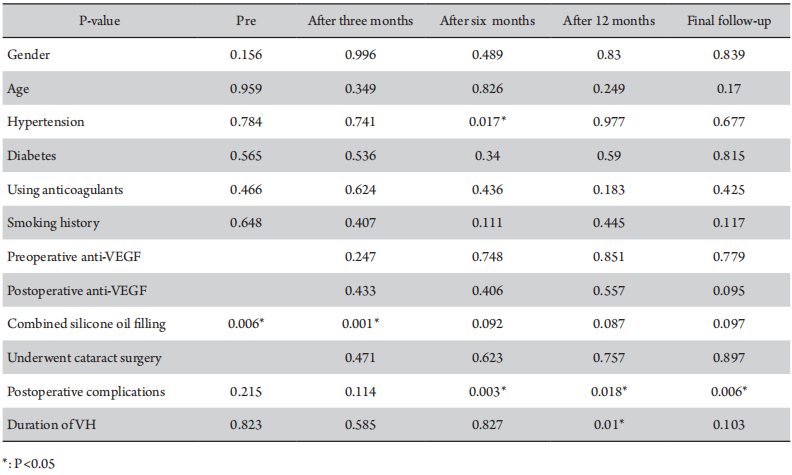
Results: The average follow-up time was 20.0±15.82 months. The average preoperative best-corrected visual acuity (BCVA) was 2.12±0.65 logarithm of the minimum angle of resolution (logMAR), the BCVA at six months was 1.65±0.64 logMAR, and the six-month follow-up BCVA was 1.67±0.76 logMAR. Compared to the average preoperative BCVA, the six-months and last follow-up BCVA after vitrectomy improved (P<0.05). The BCVA at the final follow-up was better than 1.3logMAR only in 14 eyes (28.6%). Postoperative complications were observed in 10 eyes (20.4%), including recurrent retinal detachment, recurrent vitreous hemorrhage, macular hole, hyphema and lens dislocation. Fourteen eyes (28.6%) underwent cataract surgery procedure an average of 10.16±5.14 months after vitrectomy. BCVA one week and three months after cataract surgery improved compared to BCVA before cataract surgery (P<0.05). Hypertension was associated with BCVA six months after vitrectomy (P=0.017). The BCVA at baseline and three months after PPV were worse in patients who underwent vitrectomy combined with silicone oil filling (P<0.05). Eyes with postoperative complications had worse BCVA at six months, 12 months, and at the final follow-up after PPV (P<0.05). The duration of VH is related to the BCVA12 months after PPV visual acuity after surgery. Patients who underwent vitrectomy within one month of the onset of vitreous hemorrhage had better BCVA 12 months after vitrectomy than those who underwent vitrectomy surgery one month later (P=0.015).
Conclusions: Although the prognosis of vitrectomy varies greatly, cataract surgery could be considered to improve BCVA if polypoidal lesions are inactive six months after vitrectomy.
全文
The inclusion criteria were as follows: (1) diagnosis of PCV based on the results of fundus examination, B ultrasound, optical coherence tomography (OCT), fundus fuorescein angiography (FFA), and indocyanine green angiography (ICGA), both preoperatively and postoperatively, and the presence of orange red polypoidal lesions during the operation; (2) vision loss due to PCVVHwas treated with 23-gauge PPV; and (3) the follow-up durationwas at least six months.
Similarly, the exclusion criteria were as follows: (1) traumatic vitreous hemorrhage; (2) other ocular diseases that could affect visual acuity, such as primary glaucoma, optic neuritis, age-related macular degeneration(AMD), retinal vein occlusion, choroidal melanoma, and retinal vasculitis; and (3) a medical history of photodynamic therapy(PDT) or PPV.
All patients underwent a comprehensive eye examination, including best-corrected visual acuity (BCVA), slit-lamp microscopy, and B-scan before surgery. The patients also underwent 23-gauge PPV, including central and peripheral vitrectomies, performed by multiple skilled surgeons. We used a wide-angle viewing system for PPV and identified the peripheral retina during the peripheral vitrectomy. If subretinal hemorrhage was observed during surgery without retinal tears, this was not treated due to the signifcant damage caused by clearing subretinal hemorrhage. According to the surgeon’s judgment, silicone oil or C3F8 was used to fill the vitreous cavity. In cases with retinal tears or poor fundus conditions, silicone oil is generally chosen. Epiretinal membrane enucleation was performed if a macular epiretinal membrane was observed. The following data was collected from each of the patients enrolled : BCVA before and after surgery, duration of VH until surgery, hypertension, diabetes, anticoagulant use, smoking history, anti-vascular endothelial growth factor (VEGF) use, spectrum OCT (SD-OCT; Heidelberg, Germany), postoperative complications, and secondary surgery during follow-up.
A paired t-test was used to compare the visual improvement and differences between the BCVA of post-vitrectomy at three, six, and 12 months and at the final follow-up from the BCVA of baseline pre-vitrectomy. The BCVAof post-cataract surgery at one week and three months was compared to the BCVA of baseline pre-cataract surgery performed after vitrectomy. The prognostically relevant factors were grouped, and independent sample t-tests were used to compare the differences in BCVA at each time point. One-way analysis of variance (ANOVA) was used to compare the BCVA at baseline and post-vitrectomy at three, six, and 12 months and at a final follow-up between the age groups and BCVA groups. Avalue of P≤0.05 was considered statistically significant. Statistical analyses were performed using SPSS for Windows (version 17.0; SPSS Inc., Chicago, IL, USA).
Table 1 Clinical characteristics of patients with massive vitreous hemorrhage secondary to polypoidal choroidal vasculopathy
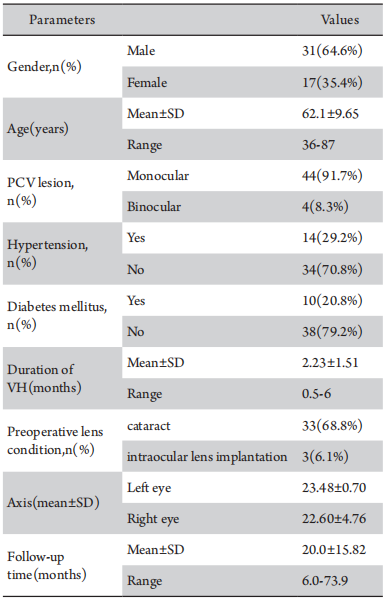
Table 2 BCVA at baseline and three, six, and 12 months final follow-up after vitrectomy
Eight eyes underwent vitrectomy combined with silicone oil flling, and the silicone oil was taken out at 11.99±6.25 months (range 3.8-25 months) after surgery. Four eyes were observed recurrent retinal detachment after removing silicone oil at 11.54±8.04 months(range 3.8-25 months).
Fourteen eyes (28.6%) were subjected to phacoemulsifcation and intraocular lens implantation in an average time of 10.16±5.14 months (range 1.97-21.43 months) after vitrectomy. Six eyes underwent vitrectomy combined with cataract surgery due to postoperative complications. Compared with the BCVA before cataract surgery, the final BCVA was stable or improved in 13 eyes, increased in one eyes. BCVA at one week and three months post-cataract surgery was improved compared with BCVA before cataract surgery (P<0.05)(Table 3). Among these 14 eyes, the BCVA at the final follow-up was better than 1.3 logMAR only in six eyes (28.6%); the fnal follow-up BCVA of two eyes improved compared with the blind standard, and the other two eyes improved compared with the low visual acuity standard.
Table 3 BCVA before cataract surgery and 1 week and 6 months after cataract surgery
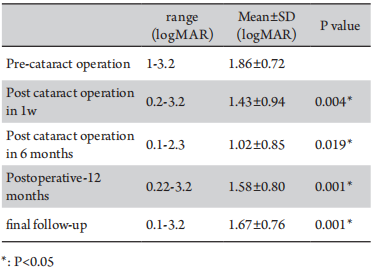
Table 4 Factors related to visual prognosis after PPV surgery
There is no consensus on the timing of surgery for patients with PCVVH or whether anti-VEGF therapy is required before surgery in the clinical setting. Some surgeons tend to inject anti-VEGF into the vitreous after the onset of vitreous hemorrhage and then perform PPV surgery after the vitreous hemorrhage is slightly reduced, which could reduce the difficulty of the operation. Chen et al.[11] reported that anti-VEGF injection into the vitreous before PPV surgery could help reduce the frequency of anti-VEGF treatments and postoperative complications and improve short-term vision after surgery. Perioperative anti-VEGF could reduce the difficulty of surgery and reduce the occurrence of postoperative complications.[11] Previous animal experiments have shown that subretinal hemorrhage lasts for seven days, causing irreversible damage to the photoreceptor cells and retinal pigment epithelial(RPE) atrophy. Subsequently, local retinal necrosis occurs within 14 days, which allows red blood cell fragments to pass through the damaged retina, causing vitreous hemorrhage.[12-13] Kimura et al.[14] proposedan optimal operation time for SMH secondary to PCV of 7-10 days after the onset of SMH. On the one hand, a premature intervention can lead to recurrent bleeding after operation. However, on the other hand, if the intervention time is too late, this can cause irreversible damage to the retina, leading to poor postoperative vision. Nevertheless, the duration of VH in the enrolled patients ranged from half to six months. Therefore, we divided them into groups according to whether the duration of VH exceeded one month or not, and found that patients who underwent vitrectomy within one month of the onset of VH had better BCVA 12 months after vitrectomy than those who underwent vitrectomyone month later (P=0.015). There was no statistically significant relation between preoperative anti-VEGF levels and BCVA(P>0.05). If PPV surgery is performed early, the retina can easily be damaged owing to a thick subretinal hemorrhage. Blood cell fragments stay in the vitreous for a long time, which may cause irreversible toxic effects on the retina, and damage the retina and RPE layer. Thus, we propose that vitrectomy surgery should be performed within one month of the onset of massive vitreous hemorrhage in order to improve vision after surgery.
PPV is theprimary treatment for PCVVH. Zhao et al.[15] retrospectively analyzed 103 eyes with PCVVH and found that BCVA was significantly better after PPV than before surgery. Lin et al.[16] studied 17 eyes with PCVVH that underwent vitrectomy, of which visual acuity improved in 16 eyes. Severe cataract and macular scarring causepoor visual acuity. In the present study, BCVA at three, six, and 12 months and at the last follow-up after vitrectomy improved compared to the average preoperative BCVA (P<0.05), consistent with the results of previous studies.[15-19] However, the visual acuity of patients with PCVVH varies considerably after vitrectomy, with most patients maintaining a low level of visual acuity. As shown in Figure 1, PCVVH is characterized by large polypoid lesions and strong activity. If the lesion does not involve the macula, the visual prognosis is better. In our study, the BCVA ranged from 0.1 logMAR to 3.2 logMAR at the final follow-up. The BCVA atthe final follow-up was better than 1.3l ogMAR only in 14 eyes (28.6%). Zhao et al.[16] found that the morrhagic retinal detachment, baseline central macular thickness, and best-corrected visual acuity were factors associated with final best-corrected visual acuity (P < 0.05) in PCV patients. Previous studies have shown that the incidence of secondary epiretinal membranes is 16.6% and that older individuals are more likely to develop an epiretinal membrane.[20] In this study, 58% of patients underwent epiretinal membrane enucleation, and the incidence of epiretinal membrane enucleation was much higher than that in the normal population. We speculate that this may be because PCV patients are mostly elderly individuals aged 50-70 years, with factors such as vitreous hemorrhage and retinal detachment exacerbating the progression of the epiretinal membrane.
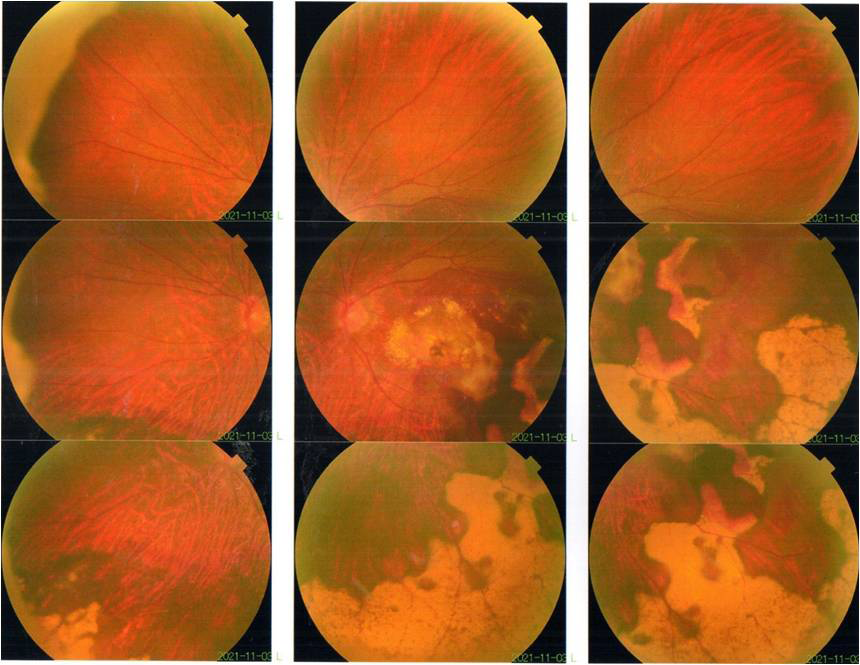
Figure 1 Fundus photography of the left eye: a large orange polypoid lesion at the posterior pole, the choroid in the inferior temporal and peripheral areas is chronic hemorrhagic foci
Common postoperative complications of PPV in patients with PCVVH include iatrogenic retinal tears, recurrent vitreous hemorrhage, complicated cataracts, hyphema, secondary glaucoma, macular subretinal fibrosis, retinal detachment, and choroidal detachment.[17,21-22] Iatrogenic retinal tearsare the most common surgical complication, with an incidence of approximately 17.8%, mostly observed during the induction of posterior vitreous detachment (PVD).[23] Studies have also reported sympathetic ophthalmia in the other eye, which is a rare postoperative complication.[23] Postoperative complications were observed in 10 eyes (20.4%) and included recurrent retinal detachment(18.4%), vitreous hemorrhage(6.1%), macular holes (2%), hyphema(6.1%), and lens dislocation(4.1%). The peak period of postoperative complications was within one year after PPV, although one patient had recurrent retinal detachment more than two years after the first PPV. Notably, recurrent retinal detachment was observed in four eyes after silicone oil removal. Therefore, choosing the appropriate time to perform the SO removal surgery is a key factor in effectively reducing postoperative complications. Postoperative complications are another heavy blow to patients, with their vision often worsening as a result. Among patients with postoperative complications, BCVA was mostly less than 1.3 logMAR.
All patients included in this single-center study were from the Zhongshan Ophthalmology Centre of Sun Yat-Sen University. Since this is a retrospective study, we hope that a prospective longitudinal study will shed further light on the prognosis and factors infuencing patients with PCVVH.
When PCV is secondary to VH, visual acuity drops sharply, for which vitrectomy is the primary clinical treatment. This studyevaluates the visual prognosis of patients with PCVVH undergoing PPV surgery and shows that PPV can improve the short- and long-term visual acuity of patients with PCVVH. However, visual acuity after PPV was found to difer signifcantly, with only 28.6% of the patients showing a better long-term visual acuity than the non-blind standard. If polypoid lesions are not active, phacoemulsification and intraocular lens implantation can be considered to improve vision approximately half a year after PPV. Although some patients had a good visual acuity after cataract surgery, up to 57.1% of their vision either did not improve or deteriorated. Postoperative complications were observed in 10 eyes (20.4%). We also found that hypertension, vitrectomy combined with silicone oil filling, postoperative adverse events, and vitreous hemorrhage lasting >1 month were associated with a poor postoperative BCVA.
Correction notice
NoneAcknowledgement
NoneAuthor Contributions
(I) Conception and design: YL(II)Administrative support: TL,BQL,YL
(III) Provision of study materials or patients: TL,BQL,YL
(IV) Collection and assembly of data: CXC and JLC
(V) Data analysis and interpretation: CXC and QW
(VI) Manuscript writing:All authors
(VII) Final approval of manuscript:All authors
Funding
This study was supported by the Bethune·Lumitin Research Funding for the young and middle-aged Ophthalmologists (grant no. BJ-LM2021014J)and the Science and Technology Program of Guangzhou, China (SL2022A03J00452).The funding organizations had no role in the following aspects: design and conduct of the study; the collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
Confict of Interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form.Patient consent for publication
Patients orally agreed to the use of their data in the present study.Ethical Statement
All experimental protocols were approved by the ethics committee of Zhongshan Ophthalmic Center (Guangzhou, China).Provenance and Peer Review
This article was a standard submission to our journal. The article has undergone peer review with ouranonymous review system.Data Sharing Statement
NoneOpenAccess Statement
This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license). See: https://creativecommons.org/licenses/by-nc-nd/4.0/.基金
参考文献
1. Kwok AH. Polypoidal choroidal vasculopathy in Chinese patients. Br J Ophthalmol, 2002, 86(8): 892-897. DOI:10.1136/bjo.86.8.892.
2. Uyama M, Wada M, Nagai Y, et al. Polypoidal choroidal vasculopathy: natural history. Am J Ophthalmol, 2002, 133(5): 639-648.
3. Hou J, Tao Y, Li XX, et al. Clinical characteristics of polypoidal choroidal vasculopathy in Chinese patients. Graefe’s Arch Clin Exp Ophthalmol, 2011, 249(7): 975-979. DOI:10.1007/s00417-010-1575-7.
4. Schulze-Bonsel K, Feltgen N, Burau H, et al. Visual acuities “hand motion” and “counting fingers” can be quantified with the Freiburg visual acuity test. Invest Ophthalmol Vis Sci, 2006, 47(3): 1236. DOI:10.1167/iovs.05-0981.
5. Lorentzen TD, Subhi Y, Sørensen TL. Prevalence of polypoidal choroidal vasculopathy in white patients with exudative age-related macular degeneration: Systematic Review and Meta-Analysis. Retina, 2018, 38(12): 2363-2371. DOI:10.1097/iae.0000000000001872.
6. Honda S, Matsumiya W, Negi A. Polypoidal choroidal vasculopathy: clinical features and genetic predisposition. Ophthalmologica, 2014, 231(2): 59-74. DOI:10.1159/000355488.
7. Kimura S, Morizane Y, Hosokawa MM, et al. Outcomes of vitrectomy combined with subretinal tissue plasminogen activator injection for submacular hemorrhage associated with polypoidal choroidal vasculopathy. Jpn J Ophthalmol, 2019, 63(5): 382-388. DOI:10.1007/s10384-019-00679-2.
8. Liu B, Lai K, Ma Y, et al. Systemic risk factors for vitreous hemorrhage secondary to polypoidal choroidal vasculopathy. Ophthalmol Ther, 2023, 12(5): 2769-2780. DOI:10.1007/s40123-023-00783-0.
9. Kawasaki R, Wang JJ, Ji GJ, et al. Prevalence and risk factors for age-related macular degeneration in an adult Japanese population the funagata study. Ophthalmology, 2008, 115(8): 1376-1381.e2. DOI:10.1016/j.ophtha.2007.11.015.
10. Kawasaki R, Wang JJ, Aung T, et al. Prevalence of age-related macular degeneration in a Malay population the Singapore Malay eye study. Ophthalmology, 2008, 115(10): 1735-1741. DOI:10.1016/j.ophtha.2008.02.012.
11. Chen L, Qu L, Gui Q, et al. Effects of anti-vascular endothelial growth factor drugs before and after pars Plana vitrectomy in patients with polypoidal choroidal vasculopathy and vitreous hemorrhage. J Ocul Pharmacol Ther, 2021, 37(10): 591-596. DOI:10.1089/jop.2021.0039.
12. Toth CA. Fibrin directs early retinal damage after experimental subretinal hemorrhage. Arch Ophthalmol, 1991, 109(5): 723. DOI:10.1001/archopht.1991.01080050139046.
13. Lincoff H. Pathogenesis of the vitreous cloud emanating from subretinal hemorrhage. Arch Ophthalmol, 2003, 121(1): 91. DOI:10.1001/archopht.121.1.91.
14. Kimura S, Morizane Y, Hosokawa M, et al. Submacular hemorrhage in polypoidal choroidal vasculopathy treated by vitrectomy and subretinal tissue plasminogen activator. Am J Ophthalmol, 2015, 159(4): 683-689.e1. DOI:10.1016/j.ajo.2014.12.020.
15. Zhao XY, Luo MY, Meng LH, et al. The incidence, characteristics, management, prognosis, and classification of breakthrough vitreous hemorrhage secondary to polypoidal choroidal vasculopathy. Retina, 2021, 41(8): 1675-1685. DOI:10.1097/iae.0000000000003098.
16. Lin HC, Yang CH, Yang CM. Visual outcomes of vitrectomy for polypoidal choroidal vasculopathy-related breakthrough vitreous haemorrhage. Eye, 2014, 28(7): 797-807. DOI:10.1038/eye.2014.124.
17. Jung JH, Lee JK, Lee JE, et al. Results of vitrectomy for breakthrough vitreous hemorrhage associated with age-related macular degeneration and polypoidal choroidal vasculopathy. Retina, 2010, 30(6): 865-873. DOI:10.1097/iae.0b013e3181c969e9.
18. Li MS, Tsen CL. Clinical features and outcomes of breakthrough vitreous hemorrhage secondary to polypoidal choroidal vasculopathy. PLoS One, 2022, 17(12): e0279778. DOI:10.1371/journal.pone.0279778.
19. Inoue N, Kato A, Araki T, et al. Visual prognosis of submacular hemorrhage secondary to age-related macular degeneration: a retrospective multicenter survey. PLoS One, 2022, 17(7): e0271447. DOI:10.1371/journal.pone.0271447.
20. Xiao W, Chen X, Yan W, et al. Prevalence and risk factors of epiretinal membranes: a systematic review and meta-analysis of population-based studies. BMJ Open, 2017, 7(9): e014644. DOI:10.1136/bmjopen-2016-014644.
21. Narayanan R, Mithal K, Jalali S, et al. Vitreous haemorrhage in massive hemorrhagic polypoidal choroidal vasculopathy: clinical characteristics and surgical outcomes. Int J Retina Vitreous, 2015, 1(1): 25. DOI:10.1186/s40942-015-0025-4.
22. Li ZX. Long-term observation of vitrectomy without subretinal hemorrhage management for massive vitreous hemorrhage secondary to polypoidal choroidal vasculopathy. Int J Ophthalmol, 2019, 12(12): 1859-1864. DOI:10.18240/ijo.2019.12.07.
23. Suetsugu T, Yasukawa T, Uemura A, et al. Sympathetic ophthalmia in fellow eye after vitrectomy for massive subretinal hemorrhage secondary to polypoidal choroidal vasculopathy. Int Med Case Rep J, 2018, 11: 293-296. DOI:10.2147/imcrj.s183836.