


HIGHTLIGHTS
1.Critical Discoveries and Outcomes
• Providing refractive correction spectacles may be a simple yet impactful intervention to alleviate depressive symptoms in highly myopic adults.
2.Methodological Innovations
• Providing refractive correction spectacles to highly myopic adults.
3. Prospective Applications and Future Directions
• Further randomized clinical trial is needed to confirm this finding. If it holds true, community-based screening for depressive symptoms coupled with targeted spectacle provision could meaningfully improve quality of life for individuals with high myopia.
Introduction
Myopia is a growing global public health concern. Projections indicate that by 2050, 50% of the world’s population will be myopic (spherical equivalent: SER ≤ -0.50D), with 10% affected by high myopia (SER≤-5.00D).[1] Prevalence is particularly high in East and Southeast Asia, where approximately 80% of young adults are myopic and 20% have high myopia.[2-3] High myopia significantly increases the risk of sight-threatening complications, including retinal detachment, myopic macular degeneration, cataracts, and open-angle glaucoma.[4] Moreover, uncorrected myopia remains a leading cause of visual impairment worldwide.[5] Studies indicate that myopia undercorrection is prevalent among adultsnin China (19.4% in Beijing; 24.9% in Shanghai), particularly among those age ≥40 years.[6-7] For an individual with -5.00D myopia, uncorrected distance visual acuity is about 6/172 Snellen (1.46 logMAR), which exceeds the World Health Organization threshold for blindness (3/60 in Snellen; 1.30 logMAR).[8] This function limitation is clinically significant, as population surveys consistently rank blindness among the most feared health outcomes, often surpassing cancer and paralysis.[9-10]
Depression represent another major global health challenge and is a leading cause of disability worldwide.[11] Depression and anxiety collectively account for an estimated 12 billion lost working days annually, translating to roughly US$1 trillion in lost productivity.[12] Epidemiological studies across diverse populations consistently demonstrate an association between visual impairment and depressive symptoms, with odds ratios ranging from 1.89 and 3.34.[13-16] Proposed mechanism include age, vision-specific distress, functional limitations secondary to vision loss, and socioeconomic determinants such as educational attainment and income.[10] Furthermore, a community-based study found that myopic individuals have a higher prevalence of depressive symptoms than non-myopic controls (OR= 1.39).[17] Given the substantial individual and societal burden of both conditions, there is a critical need to evaluate interventions that may mitigate psychological distress in high myopic populations. However, research on targeted interventions for this group remains scarce.
We hypothesize that providing full refractive correction via spectacles would reduce the prevalence of screened depressive symptoms in adults with high myopia (cycloplegic SER ≤-5.00D) .Although presbyopia commonly affects adults aged ≥40 years, this study specifically address distance visual acuity, which remains the primary functional concern for highly myopic individuals. This study aims to assess whether spectacle provision alleviate s depressive symptoms and to identify baseline factors (e.g., age, gender) associated with symptom improvement. These findings may inform integrated public health strategies and clinical care pathways that address both visual and psychological outcomes in high myopia management.
Materials and methods
Study design, setting, and participants
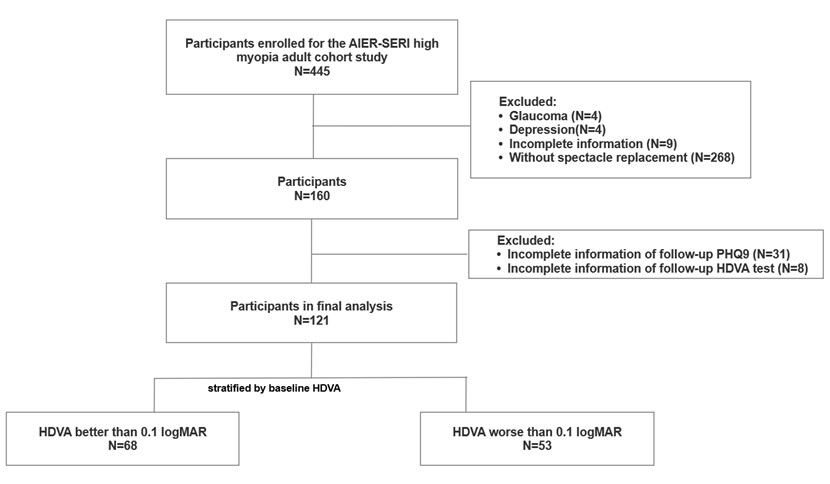
The study is component of the AIER-Singapore Eye Research Institute (SERI) High Myopia Adult Cohort Study, an ongoing community-based prospective cohort of Chinese adults with high myopia conducted in Changsha, China. Eligible participants were adults with high myopia (SER≤-5.00D) enrolled between August 2021 and December 2023. Baseline exclusion criteria included the presence of diabetic retinopathy, age-related macular degeneration, central serous chorioretinopathy, retinal vascular abnormalities, uveitis, retinitis pigmentosa, amblyopia, and glaucoma (n=4), as well as a prior diagnosis of depression or other psychiatric disorders (n=4). Incomplete baseline data led to the exclusion of 9 individuals. Additionally, participants were excluded from the final analysis if they did obtain the prescribed spectacles (n=268), failed to post-intervention Patient Health Questionnaire-9 (PHQ-9) (n=31), or missied the post-intervention visual acuity assessment (n=8)(Figure 1). The study protocol was approved by the Centralized Institutional Review Boards of the Aier Eye Hospital, Changsha (ethics approval ID: AIER2020IRB05) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
After change of spectacles, reduction of presence of depressive symptoms was observed, especially in subgroup, HDVA worse than 0.1 logMAR (p=0.03). Asterisk indicates statistically significant.
Measurements
At the baseline visit, all participants underwent a comprehensive bilateral ophthalmological examination, including slit-lamp examinations. Cycloplegic autorefraction was obtained using an autorefractor (Nidek ARK-1, Nidek Technologies, Gamagori, Japan). Habitual distant visual acuity (HDVA) was assessed monocularly and recorded in (logMAR) using tumbling E Snellen visual charts. Axial length (AL) was measured using non-contact optical biometry (Lenstar 900 instrument, Haag-Streit USA, Mason, Ohio, USA). Baseline HDVA was recorded before the provision of study spectacles. At the one-month follow-up visit, after participants received the new spectacles, HDVA was reassessed while wearing them. Baseline demographic characteristic (age, gender, ethnicity), socialeconomic status (eductional attainment), and medical history (personal and family history of systemic diseases) were collected through self-administered questionnaires.
Depressive symptoms
Depressive symptoms were assessed using Chinese version of the Patient Health Questionnaire (PHQ-9), a widely validated screening instrument.[18-20] Total PHQ-9 scores range from 0 to 27, with higher values indicating greater symptom severity. Following established criteria,[17,19-21] scores were classified into four severity levels: no symptoms (0 ≤ score ≤ 4), mild (5< score ≤ 9), moderate (10< score ≤ 14), severe (>15). A score >4 was used to define the overall presence of depressive symptoms. Assessment were conducted at baseline and again three weeks after participants received their new spectacles (approximately seven weeks post-enrollment). The PHQ-9 was self-administered, with research staff available to provide clarification if needed.
Intervention
At enrollment, all participants were offered free replacement single-vision spectacles without restrictions. The research team provided the spectacles at no cost, including to participants with good baseline HDVA. Spectacles were manufactured and dispensed within one month of the baseline examination. Upon pickup, HDVA was reassessed while participants wore the new spectacles. Depressive symptoms were reassessed three weeks after participants began wearing them.
Outcomes
The primary outcome was the change in the prevalence of depressive symptoms from baseline to post-intervention. The secondary outcome was remission of depressive symptoms, defined as the transition from a symptomatic state at baseline to an asymptomatic state following refractive correction.
Statistical analysis
Analyses were conducted at patient level. For ocular characteristics, the eye with the more severe myopia was selected for each participant. Continuous variables were reported as mean ± standard deviation (SD) and compared using the t-test. These variables were also categorized using either median splits or clinically relevant cutoffs: SER (< -7.90 D, ≥ -7.90 D), AL (≥ 26.9 mm, < 26.9 mm), HDVA (> 0.1 logMAR, ≤ 0.1 logMAR), HDVA improvement (None, < 1 line , 1-2 lines, or≥2 lines). Categorical variables were expressed as frequencies and percentages and compared using Chi-squared test. Within-subject comparisons of categorical outcome before and after intervention (e.g., changes in depressive symptom status) were assessed using McNemar’s test.
Given our hypothesis that refractive correction would reduce the prevalence of screened depressive symptoms, we conducted a subgroup annalysis stratified by baseline HDVA to account for participants who already had good visual acuity or experienced minimal improvement after correction. Participants were classified into a good HDVA group (G-HDVA; ≤ 0.1 logMAR) and a poor HDVA group (P-HDVA; > 0.1 logMAR). The distributions of HDVA improvement categories between these groups using the chi-squared test.
Associations between potential predictors (demographic, socioeconomic status, medical histories, ocular characteristics, VA improvement) and depressive symptom remission were evaluated using univariable and multivariable logistic regression models. The Final multivariable model was derived using backward elimination. As a sensitivity analysis, we also performed univariable and multivariable linear regression with change in PHQ-9 scores treated as a continuous outcome. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA). A two-sided P<0.05 was considered statistically significant.
Results
As shown in Figure 1, a total of 121 participants with highly myopia completed follow-up HDVA examinations and the PHQ-9 questionnaire after-intervention. Based on baseline HDVA, 68 participants were classified into the G-HDVA group and 53 into the P-HDVA group.
Table 1 presents the baseline distributions depressive symptom status of the cohort. The mean age was 40.3±7.4 years, and 38.0% of participants were male. The majority (93.4%) were of Han ethnicity, 87.6% had college degree or higher. Most participants reported no family history of systemic diseases (76.0%) and no personal history of systemic diseases (86.0%). The mean AL was 27.2±1.7 mm, and the mean SER was -9.07±3.91 D. At baseline, 14% of participants had MMD, and 68.6% screened positive for depressive symptoms. When comparing the G-HDVA and the P-HDVA groups, no significant differences were observed in age, gender, race, family/personal history of systemic diseases (Table 1). However, the G-HDVA group had a higher proportion of participants with a college degree or higher (94.1% vs. 79.2%, P=0.01). Compared with the G-HDVA group, the P-HDVA group had significantly longer AL (27.7±1.9 mm vs. 26.7±1.3 mm, P=0.001;≥26.9 mm: 64.2% vs. 38.2%, P=0.005), more myopic SER (-10.82±4.70 D vs. -7.71±2.42 D, P<0.001; <-7.90 D: 67.9% vs. 30.9%, P<0.001), and a higher prevalence of MMD (24.5% vs. 5.9%, P=0.003). Both groups showed similarly high rates of screened depressive symptoms at baseline (G-HDVA: 69.1%; P-HDVA: 67.9%), with no significant differences in symptom presence or severity prior to spectacle provision (Table 1).
|
Characteristics |
Overall |
Stratification by baseline HDVA (in the worse eye) |
||
|
Better than 0.1 logMAR (n=68) |
Worse than 0.1 logMAR (n=53) |
P-value |
||
|
Age (Years) |
40.3 (7.4) |
39.8 (6.2) |
40.9 (8.6) |
0.45 |
|
Age |
|
|
|
|
|
<40 years |
64 (52.9%) |
36 (52.9%) |
28 (52.8%) |
0.99 |
|
≥40 years |
57 (47.1%) |
32 (47.1%) |
25 (47.2%) |
|
|
Gender |
|
|
|
|
|
Male |
46 (38.0%) |
31 (45.6%) |
15 (28.3%) |
0.05 |
|
Female |
75 (62.0%) |
37 (54.4%) |
38 (71.7%) |
|
|
Race |
|
|
|
|
|
Han |
113 (93.4%) |
62 (91.2%) |
51 (96.2%) |
0.27 |
|
Others |
8 (6.6%) |
6 (8.8%) |
2 (3.8%) |
|
|
Education level |
|
|
|
|
|
High school or below |
15 (12.4%) |
4 (5.9%) |
11 (20.8%) |
0.01* |
|
College or above |
106 (87.6%) |
64 (94.1%) |
42 (79.2%) |
|
|
Any family history of systemic diseases (including Diabetes, Hypertension) |
|
|
|
|
|
No |
92 (76.0%) |
50 (73.5%) |
42 (79.2%) |
0.46 |
|
Yes |
29 (24.0%) |
18 (26.5%) |
11 (20.8%) |
|
|
Any systemic diseases (including Diabetes, Hypertension, Hepatitis, Hyperthyroidism) |
|
|
|
|
|
No |
104 (86.0%) |
59 (86.8%) |
45 (84.9%) |
0.77 |
|
Yes |
17 (14.0%) |
9 (13.2%) |
8 (15.1%) |
|
|
Axial length (mm) |
27.2 (1.7) |
26.7 (1.3) |
27.7 (1.9) |
0.001* |
|
Axial length |
|
|
|
|
|
≥26.9 mm |
60 (49.6%) |
26 (38.2%) |
34 (64.2%) |
0.005* |
|
<26.9 mm |
61 (50.4%) |
42 (61.8%) |
19 (35.8%) |
|
|
Spherical Equivalent (D) |
-9.07 (3.91) |
-7.71 (2.42) |
-10.82 (4.70) |
<0.001* |
|
Spherical Equivalent |
|
|
|
|
|
<-7.90 D |
57 (47.1%) |
21 (30.9%) |
36 (67.9%) |
<0.001* |
|
≥-7.90 D |
64 (52.9%) |
47 (69.1%) |
17 (32.1%) |
|
|
Myopic macular degeneration (MMD) |
|
|
|
|
|
No |
104 (86.0%) |
64 (94.1%) |
40 (75.5%) |
0.003* |
|
Yes |
17 (14.0%) |
4 (5.9%) |
13 (24.5%) |
|
|
PHQ-9 scores |
5.8 (2.9) |
5.8 (2.6) |
5.8 (3.2) |
1.00 |
|
Presence of depressive symptoms |
|
|
|
|
|
No (PHQ-9 ≤4) |
38 (31.4%) |
21 (30.9%) |
17 (32.1%) |
0.89 |
|
Yes (PHQ-9 >4) |
83 (68.6%) |
47 (69.1%) |
36 (67.9%) |
|
|
Depressive symptoms severity |
|
|
|
|
|
No depression symptoms (PHQ-9 ≤4) |
38 (31.4%) |
21 (30.9%) |
17 (32.1%) |
0.56 |
|
Mild (4 <PHQ-9 ≤9) |
71 (58.7%) |
42 (61.8%) |
29 (54.7%) |
|
|
Moderate (9 <PHQ-9 ≤14) |
11 (9.1%) |
5 (7.4%) |
6 (11.3%) |
|
|
Severe (14 <PHQ-9 ≤27) |
1 (0.8%) |
0 (0.0%) |
1 (1.9%) |
|
|
Asterisk indicates statistically significant. |
||||
As shown in Figure 2 and Table S1, the overall proportion of participants with depressive symptoms decreased from 68.6% before spectacle provision and 60.3% afterward (P=0.07). In the G-HDVA group, the proportion decreased slightly from 69.1% to 66.2% (P=0.67). In contrast, the P-HDVA group showed a significant reduction of 15.1 percentage points, from 67.9% to 52.8% (P = 0.03).
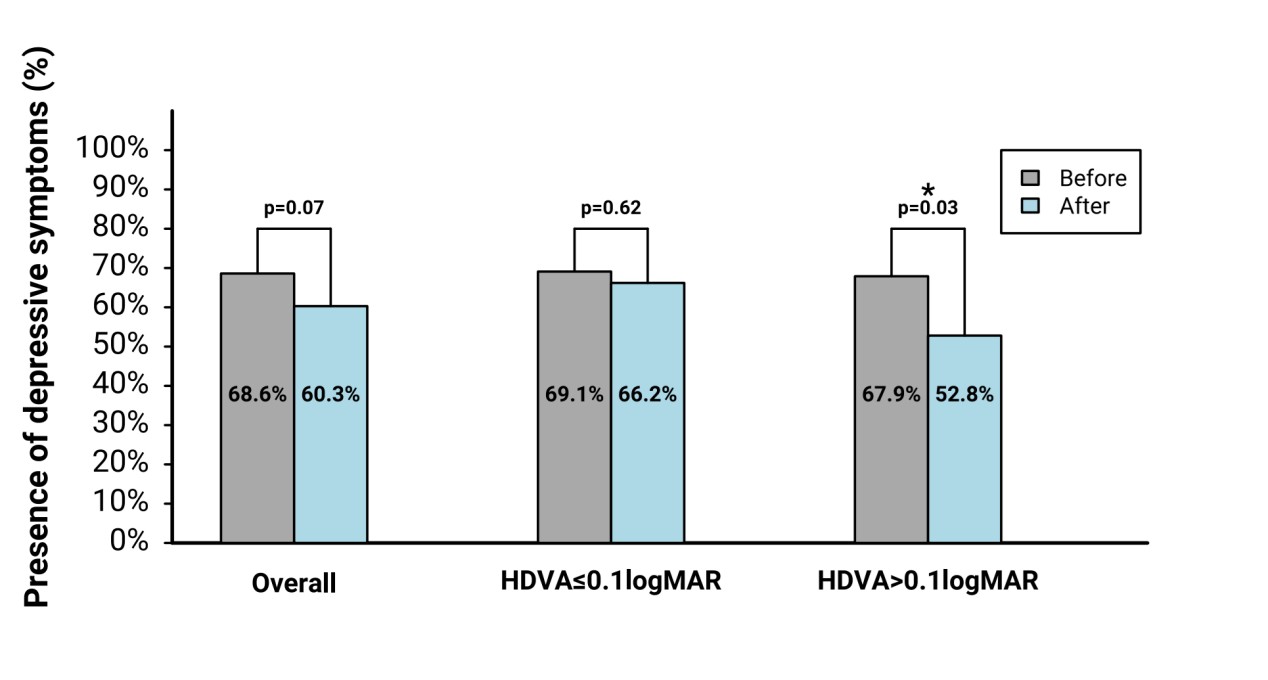
After change of spectacles, reduction of presence of depressive symptoms was observed, especially in subgroup, HDVA worse than 0.1 logMAR (P=0.03). Asterisk indicates statistically significant.
HDVA improvement after spectacles provision varied by baseline visual acuity: participants with better baseline HDVA experienced less improvement Following correction, 67.6%, 10.3%, 20.6%, and 1.5% of the G-HDVA group showed no improvement, <1-line improvement, 1–2-line improvement, and ≥2-line improvement, respectively. In the P-HDVA group, the corresponding proportions were 9.4%, 7.5%, 24.5%, and 58.5% (P< 0.001) (Figure 3). When analyzing PHQ-9 scores as a continuous outcome, the mean change was +0.3 (SD 3.2) in the G-HDVA group and −0.5 (SD 4.2) in the P-HDVA group, with no significant between-group difference (P = 0.28).
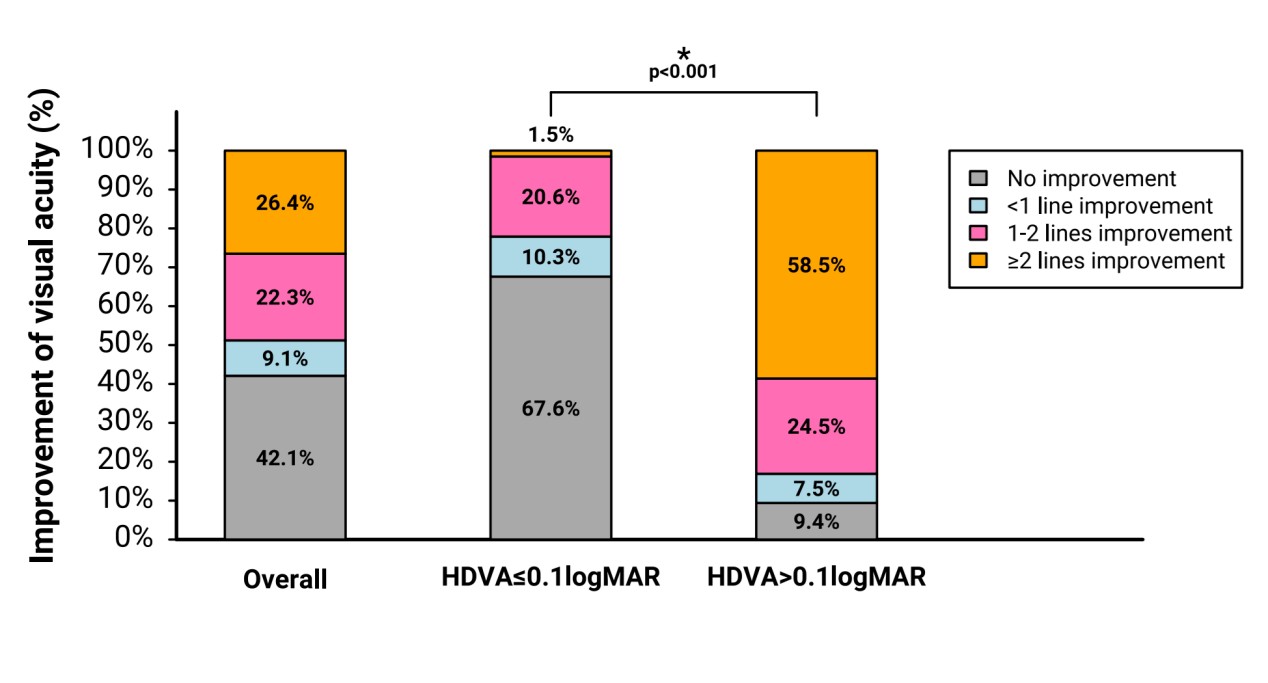
In the baseline HDVA worse than 0.1 logMAR subgroup, 90.6% showed improved HDVA≥1 line; in the baseline HDVA better than 0.1 logMAR subgroup, 22.1% showed improved HDVA≥1 line, as they had good HDVA to start with at baseline. Asterisk indicates statistically significant.
Univariable analysis was performed to assess associations between baseline characteristics, HDVA improvement, and depressive symptom remission among participants who screened positive for depressive symptoms at baseline (n=83) (Table 2). Although no variables reached statistical significance, several, trends suggested a higher likelihood of remission at follow-up among younger participants, females, those of non-Han ethnicity, individuals with lower education levels, those with a family history of systemic diseases, those without personal systemic diseases, participants with baseline HDVA > 0.1 logMAR, those with greater HDVA improvement those with AL ≥ 26.9mm (or SER < -7.90D, and those with MMD. However, no variables remained in the final multivariable model after backward elimination. A sensitivity analysis examining predictors of changes in countinuous PHQ-9 scores (n=121) is presented in Table S2. Similar directional trends were observed, but again, no predictors reached statistical significance.
|
Characteristics |
n |
n(%) Remission |
Odds ratio (95% CI) |
P-value |
|
Age |
|
|
|
|
|
<40 years |
44 |
14 (31.82%) |
Reference |
0.09 |
|
≥40 years |
39 |
6 (15.38%) |
0.39 (0.13, 1.14) |
|
|
Gender |
|
|
|
|
|
Male |
29 |
6 (20.69%) |
Reference |
0.60 |
|
Female |
54 |
14 (25.93%) |
1.34 (0.45, 3.97) |
|
|
Race |
|
|
|
|
|
Han |
76 |
17 (22.37%) |
Reference |
0.24 |
|
Others |
7 |
3 (42.86%) |
2.60 (0.53, 12.78) |
|
|
Education level |
|
|
|
|
|
high school or below |
9 |
3 (33.33%) |
Reference |
0.50 |
|
college or above |
74 |
17 (22.97%) |
0.60 (0.13, 2.64) |
|
|
Any family history of systemic diseases |
|
|
|
|
|
No |
60 |
13 (21.67%) |
Reference |
0.41 |
|
Yes |
23 |
7 (30.43%) |
1.58 (0.54, 4.66) |
|
|
Any systemic diseases |
|
|
|
|
|
No |
71 |
19 (26.76%) |
Reference |
0.20 |
|
Yes |
12 |
1 (8.33%) |
0.25 (0.03, 2.06) |
|
|
HDVA at baseline |
|
|
|
|
|
>0.1 logMAR |
36 |
11 (30.59%) |
Reference |
0.23 |
|
≤0.1 logMAR |
47 |
9 (19.15%) |
0.54 (0.20, 1.49) |
|
|
Improvement of HDVA |
|
|
|
|
|
No improvement |
33 |
5 (15.15%) |
Reference |
|
|
< 1 line improvement |
9 |
4 (44.44%) |
4.48 (0.88, 22.71) |
0.33 |
|
1-2 lines improvement |
18 |
5 (27.78%) |
2.15 (0.53, 8.76) |
|
|
At least 2 lines improvement |
23 |
6 (26.09%) |
1.98 (0.52, 7.48) |
|
|
Axial length |
|
|
|
|
|
≥26.9 mm |
42 |
13 (30.95%) |
Reference |
0.14 |
|
<26.9 mm |
41 |
7 (17.07%) |
0.46 (0.16, 1.30) |
|
|
Spherical Equivalent |
|
|
|
|
|
<-7.90 D |
38 |
11 (28.95%) |
Reference |
0.34 |
|
≥-7.90 D |
45 |
9 (20.00%) |
0.61 (0.22, 1.69) |
|
|
Myopic macular degeneration (MMD) |
|
|
|
|
|
No |
72 |
16 (22.22%) |
Reference |
0.31 |
|
Yes |
11 |
4 (36.36%) |
2.00 (0.52, 7.70) |
Discussion
In this prospective cohort study, we examined the impact of refractive correction spectacles on the prevalence of screened depressive symptoms among community-dwelling adults with high myopia in China. Updating spectacles for participants with HDVA worse than 0.1 logMAR was associated with a significant reduction in depressive symptoms, with the prevalence dropping from 67.9% to 52.8% (P=0.03). However, the single-arm design limits causal inference, and these findings should be interpreted with caution. While our results suggest that refractive correction may alleviate depressive symptoms in adults with high myopia, confirmation through randomized controlled trials is needed.
To our knowledge, this is the first study to evaluate the effect of spectacle provision on depressive symptoms in a cohort of highly myopic individuals. Our findings align with those of Owsley et al., who reported that providing spectacles to nursing home residents with uncorrected refractive error improved their vision-specific quality of life and reduced depressive symptoms.[22] Similarly, correcting refractive error in visually impaired children has been shown to improve mental health and quality of life.[23] Refractive surgeries for myopia, including LASIK, SMILE, or ICL implantation, have likewise been associated with enhanced quality of life.[24-26] In our study, the reduction in depressive symptoms was particularly pronounced among participants with P-HDVA. We attribute this to the greater improvement in HDVA within this subgroup, where 58.5% gained at least two lines of acuity. In contrast, only 32.4% of the G-HDVA group exhibited HDVA improvemnet, which may have obscured any intervention effecf on depressive symptom in this group.
Depressive symptoms were highly prevalent at baseline in our sample. We identified only one prior study reporting depressive symptom prevalence among highly myopic adults (SER≤-6.00D) in China, which found a rate of 8.0% using the same PHQ-9 questionnaire .[17] Using the Hospital Anxiety and Depression Scale (cutoff≥8), a Japanese cohort reported a prevalence of 22% among individuals with high myopia (AL≥26.5mm).[27] Our observed prevalence was substantially higher than in these previous reports; the reason for this discrepancy remain unclear. Potential explanations include our non–population-based sampling frame and the fact that most participants were undercorrected at baseline (60% had baseline HDVA > 0.0 logMAR). Regardless of these differences, the high burden of depressive symptoms in highly myopic patients is concerning. Beyound the well-documented risk of visual impairment, these patients appear vulnerable to depression, which can further compromise daily functioning and productivity.
Providing updated refractive correction may alleviate depressive symptoms ,likely because improved vision function alters patients' perceptions of their condition. Notably, a disconnect often exist between clinicians’ focus on best-corrected visual acuity and patients’ real-world experiences with habitual uncorrected vision, such as struggling to locate glasses upon waking or navigating rountine tasks without clear sight. This gap may explain why patients frequently report quality-of-life gains after refractive surgery, even when their vision is already adequately corrected with spectacles. To better understand the mental health burden in high myopia, future work should explore patients' subjective experiences of vision, vision-related function, and illness perceptions.[10] Such insights would provide esseential context for addressing the psychological challenges of this condition. Qualitative studies are therefore warranted to elucidate the factors driving the elevated rates of depressive symptoms in this population.
Given that myopia and depression represent major public health challenges with projected increases in prevalence, [28-31] our finding that spectacles provision reduces depressive symptoms in highly myopic patients with P-HDVA supports the implementation of accessible, cost-effective interventions. In clinical practice, ophthalmologists and optometrists should adopt a patient-centered approach that prioritizes optimal visual outcomes and mental well-being, including timely referrals when indicated From a public health standpoint, community-based screening for depressive symptoms coupled with targeted spectacle provision could meaningfully improve quality of life for individuals with high myopia. Patient education regarding disease progression and management may further alleviate anxiety and promote overall psychological well-being.
This is the first study to evaluate the impact of refractive correction spectacles on depressive symptoms in highly myopic adults..The approach used here, routine PHQ-9 screening followed by spectacle replacement, could be readily integrated into clinical practice and potentially benefit a large number of patients. Several limitations warrant mention. First, the single-arm design precludes causal inference; controlled trials are needed to validate these preliminary findings. Second, the sample size for analyzing predictors of depressive symptom remission was limited (only 20 out of 83 participants with baseline depressive symptoms transitioned to a non-symptomatic state), reducing the statistical power to identify significant risk factors.Larger cohort will be necessary to draw more robust conclusions. Third, because all participants received updated spectacles, we could not directly compare symptom trajectories with an untreated group. However, in the absence of intervention, we would expect depressive symptoms to remain relatively stable. Furthermore, no significant differences in baseline characteristics were observed between participants and non-participants, mitigating concerns about selection bias. Finally, the PHQ-9 depressive symptoms rather than diagnosing clinical depression; future studies employing comprehensive psychiatric evaluations are needed to confirm these results.
Conclusion
In this study, updating spectacles for participants with habitual distant visual acuity (HDVA) worse than 0.1 logMAR led to a significant reduction in depressive symptoms, representing 15.1 percentage-point cecrease. Provision of refractive correction may therefore serve as a straightforward and effective intervention to alleviate depressive symptoms in highly myopic adults. However, further randomized controlled trials are warranted to confirm these findings.
Correction notice
None
Acknowledgements
None
Author Contributions
(I) Conception and design: Weizhong Lan, Ecosse L. Lamoureux, Seang-Mei Saw, Wei Pan
(II) Administrative support: Weizhong Lan
(III) Provision of study materials or patients: Wei Pan, Xinzhe An, Dongmei Wang, Ziqi Hu, Yanfeng Jiang, Huanhuan Tan, Shuzhen Wu
(IV) Collection and assembly of data: Wei Pan, Xinzhe An, Dongmei Wang; Ziqi Hu, Yanfeng Jiang, Huanhuan Tan, Shuzhen Wu
(V) Data analysis and interpretation: Wei Pan, Xinzhe An, Dongmei, Wang, Ryan EK Man, Eva K, Fenwick
(VI) Manuscript writing: Wei Pan
(VII) Final approval of manuscript: All authors
Conflict of Interests
None of the authors has any conflicts of interest to disclose.All authors have declared in the completed the ICMJE uniform disclosure form.
Patient consent for publication
Written informed consent was obtained from all subjects
Ethics approval and consent to participate
The study obtained ethics approval from the Centralized Institutional Review Boards of the Aier Eye Hospital, Changsha (ethics approval ID: AIER2020IRB05) and was conducted in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from all subjects.
Data availability statement
The data that support the findings of this study are not openly available due to reasons of confidentiality. Upon reasonable request, deidentified data can be accessed. Please contact primary corresponding author, Prof. Weizhong Lan (lanweizhong@aierchina.com).
Open access
This is an Open Access article distributed in accordance with the Creative Commons AttributionNonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license).
Supplementary Material
|
Characteristics |
Before |
After |
P-value |
|
Presence of depressive symptoms |
|
|
|
|
Overall (n=121) |
|
|
|
|
No |
38 (31.4%) |
48 (39.7%) |
0.07 |
|
Yes |
83 (68.6%) |
73 (60.3%) |
|
|
|
|
|
|
|
HDVA better than 0.1 LogMar (n=68) |
|
|
|
|
Presence of depressive symptoms |
|
|
|
|
No |
21 (30.9%) |
23 (33.8%) |
0.62 |
|
Yes |
47 (69.1%) |
45 (66.2%) |
|
|
|
|
|
|
|
HDVA worse than 0.1 LogMar (n=53) |
|
|
|
|
Presence of depressive symptoms |
|
|
|
|
No |
17 (32.1%) |
25 (47.2%) |
0.03* |
|
Yes |
36 (67.9%) |
28 (52.8%) |
|
|
Asterisk indicates statistically significant. |
|||
|
Characteristics |
n |
Beta (95% CI) |
P-value |
|
Age |
|
|
|
|
<40 years |
64 |
Reference |
0.74 |
|
≥40 years |
57 |
0.22 (-1.09, 1.53) |
|
|
Gender |
|
|
|
|
Male |
46 |
Reference |
0.48 |
|
Female |
75 |
-0.48 (-1.83, 0.86) |
|
|
Race |
|
|
|
|
Han |
113 |
Reference |
0.46 |
|
Others |
8 |
-0.98 (-3.61, 1.64) |
|
|
Education level |
|
|
|
|
high school or below |
15 |
Reference |
0.28 |
|
college or above |
105 |
-1.08 (-3.06, 0.89) |
|
|
Any family history of systemic diseases |
|
|
|
|
No |
92 |
Reference |
0.46 |
|
Yes |
29 |
-0.57 (-2.10, 0.96) |
|
|
Any systemic diseases |
|
|
|
|
No |
104 |
Reference |
0.09 |
|
Yes |
17 |
1.60 (-0.26, 3.46) |
|
|
HDVA at baseline |
|
|
|
|
>0.1 LogMar |
53 |
Reference |
0.26 |
|
≤0.1 LogMar |
68 |
0.76 (-0.55, 2.07) |
|
|
Improvement of HDVA |
|
|
|
|
No improvement |
51 |
Reference |
|
|
< 1 line improvement |
11 |
-1.91 (-4.25, 0.42) |
0.055 |
|
1-2 lines improvement |
27 |
-2.23 (-3.90, -0.56) |
|
|
At least 2 lines improvement |
32 |
-0.89 (-2.47, 0.70) |
|
|
Axial length |
|
|
|
|
≥26.9 mm |
60 |
Reference |
0.62 |
|
<26.9 mm |
61 |
0.33 (-0.97, 1.64) |
|
|
Sphereical Equivalent |
|
|
|
|
<-7.90 D |
57 |
Reference |
0.95 |
|
≥-7.90 D |
64 |
0.04 (-1.27, 1.35) |
|
|
Myopic macular degeneration (MMD) |
|
|
|
|
No |
104 |
Reference |
0.75 |
|
Yes |
17 |
0.30 (-1.58, 2.18) |