


HIGHLIGHTS
1. Critical Discoveries and Outcomes
• A rare case of bilateral demyelinating optic neuritis (DON) following COVID-19 is reported, presenting with severe visual loss and typical imaging features, with full recovery achieved after timely treatment.
2. Methodological Innovations
• The study integrates clinical, immunological, and imaging data with literature to validate the link betweenSARS-CoV-2 and optic neuritis.
3. Prospective Applications and Future Directions
• A mixed pathogenic model (viral, immune, vascular) is proposed to facilitate early diagnosis and standardized management of this complication.
The novel coronavirus, SARS-CoV-2, emerged in late 2019 and triggered a global pandemic with diverse clinical manifestations. Initially recognized as primarily a respiratory disease, it is now known to affect multiple organ systems, including the cardiovascular, renal, neurological, and ocular systems. Optic neuritis (ON), a rare but severe neurological complication, has become an increasing concern in the context of COVID-19. ON is broadly classified into infectious and non-infectious types, with non-infectious forms more frequently encountered in clinical practice. Recognized subtypes include idiopathic demyelinating ON (IDON), multiple sclerosis-related optic neuritis (MS-ON), neuromyelitis optica spectrum disorder-related optic neuritis (NMOSD-ON), MOG antibody-associated ON (MOG-ON), chronic relapsing inflammatory optic neuropathy (CRION), and unclassified optic neuritis.[1] NMOSD-ON is particularly prevalent in Asian populations, accounting for 24%–48% of ON cases in this group.[2] Diagnosing acute ON requires a comprehensive evaluation, including clinical history, ophthalmic examination, lab testing, and cranio-orbital MRI. Acute-phase management typically involves intravenous corticosteroid pulse therapy, sometimes combined with immunosuppressants, along with supportive care. Acute demyelinating optic neuritis (DON) usually presents with unilateral vision loss and is a leading cause of visual impairment in young and middle-aged adults. Bilateral DON is particularly severe and warrants prompt clinical attention. The relationship between COVID-19 and DON remains poorly understood, particularly regarding its underlying mechanisms. We report a rare case of bilateral DON following SARS-CoV-2 infection to contribute to current evidence on neurological effects of the virus. This report discusses potential pathogenic mechanisms, reviews treatment strategies, and outlines directions for future research to improve clinical management.
Case Report
A 45-year-old woman presented with sudden bilateral vision loss, visual field defects, headache, and pain with eye movement. One week prior, she developed fever, headache, and loss of taste and smell. Nucleic acid testing confirmed SARS-CoV-2 infection, but serological antibody tests were negative, precluding viral subtyping. During her illness, she reported prolonged screen time and poor sleep quality. Ophthalmic examination revealed uncorrected visual acuity of hand motion at 50 cm bilaterally, with no improvement on refraction. A right relative afferent pupillary defect (RAPD) was present. Fundus examination showed marked bilateral optic disc edema with blurred margins and hyperemia, without retinal hemorrhages. Optical coherence tomography (OCT) confirmed significant disc swelling, with average retinal nerve fiber layer (RNFL) thickness measuring 184 μm in the right eye and 218 μm in the left eye. Due to severe vision loss, formal assessment of ganglion cell complex, visual fields, color vision, and contrast sensitivity was not possible at presentation. Orbital MRI demonstrated bilateral optic nerve thickening and contrast enhancement, predominantly in the posterior segments, with marked enhancement of the left intracranial optical nerve. (Figure 1) The optic chiasm appeared normal. Lumbar puncture was deferred due to her clinical stability, absence of other central nervous system signs, and potential risks following recent SARS-CoV-2 infection. Serum testing for MOG and AQP4 antibodies was performed; however, the absence of CSF analysis may reduce test sensitivity. Routine laboratory tests showed mild thrombocytosis (369 × 109/L; reference: 125×109/L–350×109/L), with all other parameters within normal limits. Immunological tests revealed decreased total T cells (CD3+: 53.34%; reference: 55.00%–84.00%) and CD4+ T cells (25.31%; reference: 27.00%–51.00%), slightly elevated natural killer (NK) cells (CD56+CD16+: 27.13%; reference: 5.00%–27.00%), and normal B lymphocyte counts. Anti-RNP antibodies were positive, whereas MOG, AQP4, and GFAP antibodies were negative. Following exclusion of infectious etiologies, a diagnosis of acute demyelinating optic neuritis (DON) was established. Treatment consisted of intravenous methylprednisolone (IVMP) pulse therapy (1 g daily for 3 days), followed by an oral corticosteroid taper, alongside adjunctive neurotrophic and supportive medications (idebenone, aspirin, vitamin B complex, and piracetam). By day 3, best-corrected visual acuity (BCVA) improved to 20/1,000 (right) and 20/200 (left). At day 14, BCVA further improved to 20/32 (right) and 20/25 (left), with partial resolution of visual field defects. At the one-month follow-up, optic disc edema had resolved, and RNFL thickness decreased to 123 μm (right) and 107 μm (left). Repeat orbital MRI showed no residual optic nerve enhancement. Macular thickness normalized. Although mild color vision deficits persisted, they showed gradual improvement. Contrast sensitivity was fully restored in the right eye and partially recovered at low spatial frequencies in the left eye.
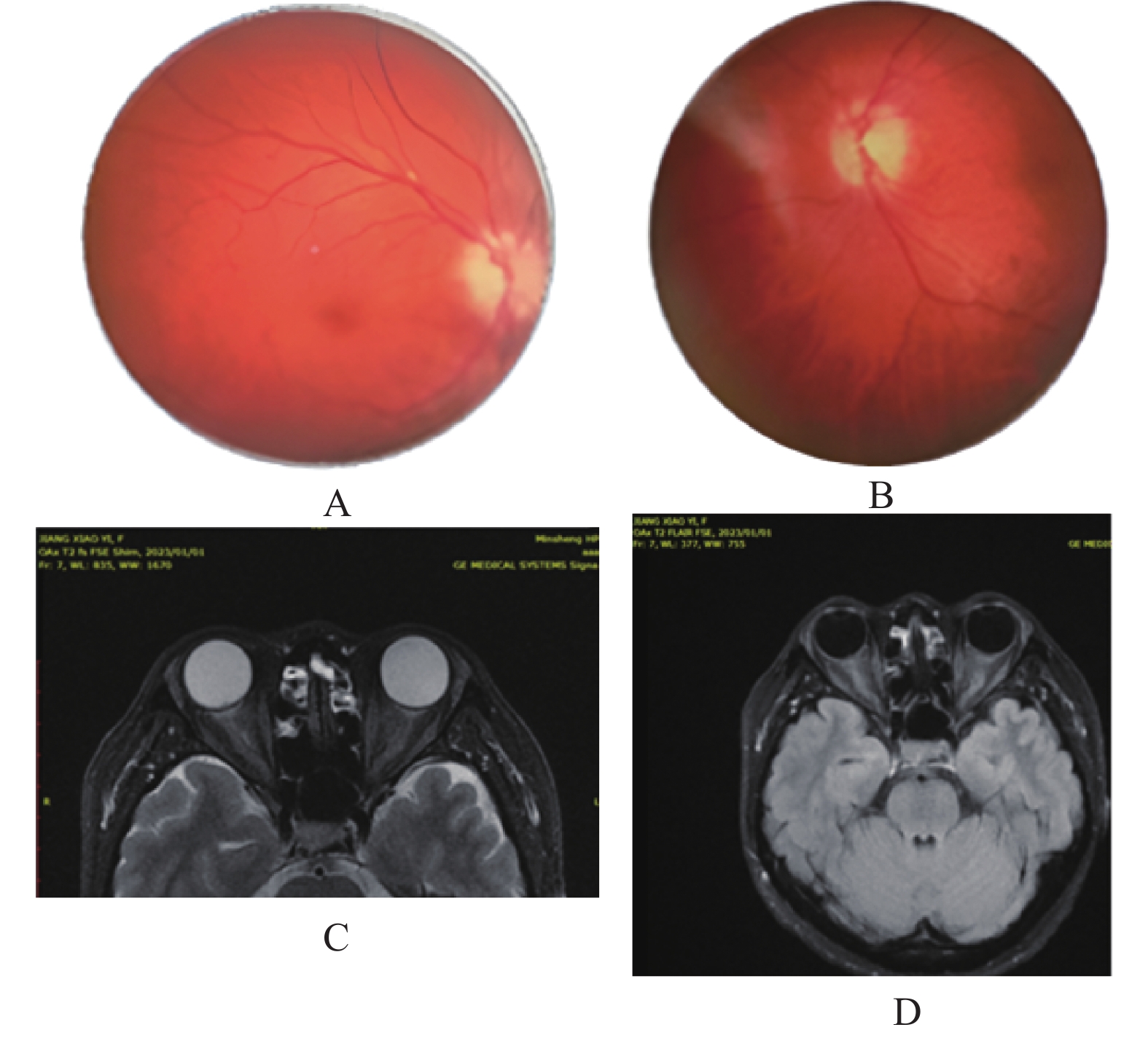
Bilateral optic disc edema, BCVA OU: HM/50 cm. Orbital MRI revealing bilateral orbital intra-segment and long-segment optic nerve thickening, marked enhancement.
Discussion
Since its emergence, SARS-CoV-2 has caused a multisystem disease that extends well beyond the respiratory tract, affecting the cardiovascular, neurological, and ocular systems. ON has emerged as a notable neurological and ocular complication. We describe a case of bilateral acute DON in a 45-year-old Asian woman following SARS-CoV-2 infection. The case is notable for negative MOG and AQP4 antibodies and a distinct immune profile, including reduced T cells, elevated NK cells, and positive anti-RNP antibodies. Although similar cases have been reported in the literature,[3-6] our case provides more comprehensive immunological and imaging data. Studies suggest that the overall prevalence of neuromyelitis optica spectrum disorder (NMOSD) remained stable during the pandemic. However, social isolation and limited healthcare access may have affected diagnosis and reporting.[7-9] SARS-CoV-2 may trigger NMOSD relapses or new-onset disease, particularly in AQP4-IgG-positive patients, likely through immune dysregulation.[7] Data on MOG-IgG-positive cases are limited, but several case reports describe post-infection optic neuritis or myelitis, suggesting a possible association with SARS-CoV-2.[10] Post-COVID-19 bilateral optic neuritis is increasingly recognized.[4,6,10-12] However, distinguishing it from MOG-ON remains clinically important, particularly given the patient’s favorable response to treatment. Some patients with MOG-ON initially test negative for antibodies, with seroconversion occurring later or requiring more sensitive assays.[13-14] This highlights the need for follow-up testing in seronegative cases. Early reports, such as a case from a Spanish hospital, described demyelinating ON in a patient recovering from COVID-19, suggesting an immune-mediated mechanism, although detailed ophthalmic findings were limited.[3] Zhou et al.[4] reported a case of bilateral vision loss with MOG-IgG positivity that improved with corticosteroid therapy, further suggesting a potential link between SARS-CoV-2 and MOG-ON. Novi et al.[5] described a 64-year-old woman who developed bilateral vision loss and sensory symptoms after infection. Despite negative AQP4 and MOG antibodies, her condition improved with steroids. Similarly, Sawalha et al.[6] reported a 44-year-old man with rapid bilateral vision loss who tested positive for MOG antibodies and showed marked improvement after methylprednisolone treatment. These reported cases share key clinical features with our patients, including acute bilateral vision loss, pain with eye movement, RAPD, optic disc edema, optic nerve enhancement on MRI, and a favorable response to corticosteroids. Together, these findings support a genuine association between SARS-CoV-2 infection and acute demyelinating optic neuritis.
Potential pathogenic model
The pathogenesis of COVID-19-associated optic neuritis is multifactorial, likely involing direct viral invasion, immune dysregulation, and vascular dysfunction. Our patient's clinical and laboratory finding support a combined pathogenic model, which differs from classic demyelinating disorders. Unlike MS-ON, which is more common in Caucasians populations and frequently associated with cerebrospinal fluid oligoclonal bands, our patient exhibited reduced CD3+ (53.34%; reference: 55.00%–84.00%) and CD4+ T cells (25.31%; reference: 27.00%–51.00%), elevated NK cells (27.13%; reference: 5.00%–27.00%), and positive anti-RNP ·antibodies. This profile differs from previously reported cases of COVID-19-associated ON, which typically show low lymphocytes and variable NK cell counts but rarely feature anti-RNP positivity.[12,15-18] This distinct immune response may result from molecular mimicry, in which SARS-CoV-2 proteins share structural similarities with optic nerve antigens.[19-20] Comprehensive antinuclear antibody (ANA) testing revealed low-titer anti-RNP antibodies without clinical or serological evidence of systemic lupus erythematosus or other connective tissue diseases. This isolated finding suggests a post-infectious immune-mediated mechanism that warrants further investigation. Direct viral neuroinvasion is also plausible, as ACE2 receptors are expressed on retinal ganglion cells and optic nerve glial cells.[21-22] This pathway is not typically involved in other demyelinating diseases. The patient’s orbital MRI demonstrated bilateral optic nerve thickening and contrast enhancement, consisted with acute inflammatory or demyelinating lesions.[13,23] Animal models indicate that SARS-CoV-2 can spread along neural pathways to central structures such as optic chiasm,[23] confirming its neurotropic potential. Vascular involvement may also contribute to the pathogenesis. The patient's mild thrombocytosis (369 × 109/L; reference: 125 × 109/L–350 × 109/L) raises the possibility of microthrombotic events, similar to mechanisms proposed in non-arteritic anterior ischemic optic neuropathy (NAION).[24-25] Together, these infectious, immune-mediated, and vascular factors highlight the need for a comprehensive diagnostic evaluation. However, establishing a definitive causal relationship requires further clinical and experimental studies.
Comparison with existing literature
Previous reports have described optic neuritis following SARS-CoV-2 infection, including MOG-IgG-positive cases[4,6] and seronegative cases.[5] However, most lack comprehensive immunological and imaging data. Our case of bilateral acute DON with negative MOG and AQP4 antibodies suggests a distinct clinical subtype potentially driven by specific immune pathways.[10-12,26-28] The detection of anti-RNP antibodies, though uncommon in this contect, supports the inclusion of broader autoimmue screening in clinical practice. Symptom onset 1–2 weeks after infection is consistent with previous reports,[3-6] indicating the post-acute phase as a critical period for immune-related complications. The patient’s rapid visual improvement following corticosteroid therapy (best-corrected visual acuity improved to 20/32 and 20/25 by day 14) highlights the importance of early treatment and provides practical guidance for managing neurological complications after COVID-19.
To place our findings in context, we compared our case with 15 recent studies (published within the last 10 years) on optic neuritis associated with COVID-19 or its vaccines (Table 1). These studies, mostly case reports or small case series, used clinical exams, OCT, MRI, visual field tests, and antibody panels. Treatment usually involved IVMP followed by an oral steroid taper. In refractory cases, plasma exchange or immunoglobulins was sometimes added. Outcomes varied from full recovery to persistent visual deficits. Most authors suggested immune-mediated mechanisms, such as molecular mimicry or direct viral damage to nerves.
|
Literature (Author, Year) |
Study Design |
Methods |
Results |
Discussion |
Comparison to Current Study |
|
Jain et al., 2024 |
Case report |
Clinical exam, OCT, perimetry, MRI, blood tests; IVMP followed by oral prednisolone |
Vision improved from finger counting to 6/9; optic disc edema resolved |
Immune-mediated demyelination; early steroid treatment key |
Similar steroid response; our case bilateral, older female, with unique immune markers |
|
Roy et al., 2024 |
Case series & review |
PubMed/Scopus review; serostatus classification; steroids ± plasma exchange |
52/54 cases improved; onset <1 month post-vaccination |
Rare vaccine side effect; needs pathophysiological study |
Vaccine-related vs. our infection-triggered case; both show steroid efficacy |
|
Duran & Aykaç, 2023 |
Case report |
Clinical exam, OCT, FFA, visual field, MRI; IVMP then oral steroids |
Vision to 20/32; disc edema reduced |
Possible viral or immune trigger; steroid-responsive |
Similar female patient, but unilateral; our case adds immunological depth |
|
Jossy et al., 2022 |
Case series |
Clinical diagnosis, labs, MRI, VEP; IVMP per ONTT protocol |
All cases improved; one MOG+ recurrence |
Neurotropism, molecular mimicry; good steroid response |
Mixed uni/bilateral vs. our antibody-negative bilateral; similar immune focus |
|
El Otmani et al., 2021 |
Case report & meta-analysis |
Case description; PRISMA meta-analysis; IVMP then oral prednisone |
Partial vision recovery; females, left eye bias |
Autoimmune inflammation; possible MS link |
Unilateral vs. our bilateral; our case adds immune details |
|
Kumar et al., 2023 |
Case report |
Clinical exam, OCT, HVF, MRI, labs; IVMP then taper |
Full symptom resolution |
Autoimmune reaction post-infection/vaccination |
Combined trigger vs. our infection-only; similar rapid steroid response |
|
Feizi et al., 2023 |
Case series |
Clinical exams, perimetry, MRI, labs; IVMP, prednisone, plasmapheresis |
Most improved; some residual deficits |
Vaccine-induced autoimmunity; monitor for demyelinating diseases |
Vaccine-related vs. our infection case; similar treatments |
|
Dutta et al., 2023 |
Case series |
Clinical exam, MRI, VEP, CSF analysis; IVMP then prednisone |
Partial to good recovery |
Molecular mimicry, cytokine storm; para/post-infectious |
Pediatric cases vs. our adult; both antibody-negative, steroid-responsive |
|
Sawalha et al., 2020 |
Case report |
Clinical exam, MRI, lumbar puncture, labs; IVMP then taper |
Near-complete recovery |
Immune-mediated; possible MOGAD trigger |
MOG+ bilateral vs. our negative; both steroid-responsive |
|
Zhou et al., 2020 |
Case report |
Clinical exam, MRI, MOG+ labs; steroid therapy |
Significant improvement |
COVID-19-MOG demyelination link |
MOG+ vs. our negative; both bilateral, steroid-responsive |
|
Novi et al., 2020 |
Case report |
Clinical exam, MRI, CSF; steroids |
Steroid-responsive |
Immune-mediated disorder |
ADEM with ON vs. our pure ON; both antibody-negative |
|
Arnao et al., 2022 |
Case report |
Clinical exam, MRI; IVMP |
Obvious improvement |
Vaccine-triggered immunity |
Vaccine vs. our infection; similar bilateral, negative antibodies |
|
Behera et al., 2022 |
Case report |
Clinical exam, MRI, labs; IVMP then prednisone |
6-month recovery |
Post-infectious demyelination |
Bilateral, negative antibodies; added facial palsy vs. our case |
|
Kivanany et al., 2022 |
Case report |
Clinical exam, MRI, AQP4+ labs; IVMP, plasma exchange |
No significant improvement |
AQP4-related post-infection |
AQP4+ vs. our negative; poor response vs. our good outcome |
|
Jossy et al., 2022 |
Case series & review |
Clinical exams, labs, imaging; steroids |
Variable improvements |
Rare neuro-ophthalmic issue; inflammatory trigger |
Similar rarity; our case adds detailed immunology |
Sigh et al. (2024),[29] reported a unilateral case of post-COVID-19 optic neuritis. Using OCT, perimetry, and MRI, they showed that steroid therapy improved vision from finger counting to 6/9. Like our case, they emphasized immune-mediated damage and early treatment, but our patient had bilateral involvement and distinct immune markers, including low T-cell counts and positive anti-RNP antibodies. Etemadifar et al. (2024)[30] reviewed vaccine-related cases and noted that most patients improved with steroids, though they called for further research into the underlying causes. While their review focused on vaccines and our case on infection, both highlight a strong response to steroid therapy. Duran and Aykaç (2023)[10] described a unilateral case in a younger woman whose vision improved to 20/32 after steroid treatment. They suggested viral or immune triggers, similar to our case, but our report provides more detailed immunological and vascular findings. Jossy et al. (2022)[31] reported a series of mixed unilateral and bilateral cases. All patients improved with steroids, and one MOG-positive case had a recurrence. Their work focuses on immune mechanisms but differs in antibody profiles. In contrast, our bilateral case provides a more detailed analysis of immune markers. Sawalha et al. (2020)[6] and Zhou et al. (2020)[4] reported MOG-positive bilateral cases, which contrast with our antibody-negative findings. Novi et al. (2020),[5] Arnao et al. (2022),[26] Behera et al. (2022),[27] Kivanany et al. (2022),[28] reported on related conditions, including ADEM, vaccine triggers, and AQP4-positive cases. Our case stands out for its detailed immune profile (low T cells, high NK cells, and positive anti-RNP antibodies) and vascular findings (elevated platelets). These results suggest the need for broader testing and further research into how immune and vascular factors may interact in this condition.
Diagnostic and therapeutic strategies
This case highlights the need for advanced diagnostic tools for COVID-19-associated optic neuritis. In addition to standard OCT and MRI,[32]single-cell sequencing of optic nerve tissue or CSF could map immune cell dynamics and clarify T cells and NK cells in inflammation.[33] This approach addresses both inflammatory and vascular factors, consistent with current guidelines for infection-related ON.[1,13-14] For treatment, IVMP pulse therapy (1 g daily for 3 days), as used in this case, remains the first-line option, followed by an oral taper to control inflammation. Plasma exchange or IVIG can be used for patients who do not respond to steroids. The 2021 Chinese Guidelines recommend early IVMP for severe or bilateral IDON, with a prolonged taper for non-IDON or multiple sclerosis to prevent recurrence.[1] Globally, glucocorticoid pulse therapy is recommended for NMOSD flares, but it should be used cautiously during active viral infections to avoid complications.[13-14] Our patient showed rapid visual improvement (20/32 and 20/25 by day 14), with resolution of optic disc edema and normalization of MRI findings within one month, demonstrating the effectiveness of early steroid therapy. Supportive treatments, including idebenone, aspirin, vitamin B, and piracetam, likely promoted nerve and vascular repair, contributing to RNFL recovery (123 μm right, 107 μm left). Visual recovery after post-infectious optic neuritis occurs in 60%–70% of cases, but residual deficits are common.[26-28] Despite minor remaining deficits, our patient achieved near-normal visual fields and improved color vision, indicating a favorable outcome. COVID-19-associated optic neuritis trends to be more severe in younger adults and patients with severe systemic illness, likely due to an exaggerated immune response.[18] MRI enhancement and low oligoclonal band positivity distinguish this condition from MS-ON, suggesting a distinct immune mechanism. When multisystem involvement occurs, such as encephalitis, comprehensive neurological evaluating is essential. Current research faces several limitations, including retrospective study designs, inconsistent antibody testing, and short follow-up periods, which make it difficult to establish causality and assess recurrence risks. The immune (low T cells, elevated NK cells) and vascular (thrombocytosis) findings in our case suggest that targeted therapies, such as JAK inhibitors (e.g., tofacitinib),[34-35] warrant further investigation, though clinical trials are needed to confirm their safety and efficacy.
Proposed research directions
Establishing a direct causal link between COVID-19 and optic neuritis remains challenging. Some cases may result from post-infectious immune dysregulation rather than direct viral invasion, making it essential to rule out alternative causes, such as latent infections or vaccine-related reactions. We propose using transgenic animal models expressing human ACE2 receptors to investigate direct optic nerve infection.[36] Such models could help verify neuronal spread and identify potential biomarkers, including serum GFAP and neurofilament light chain. Large-scale multicenter studies integrating genome-wide association studies (GWAS) and multi-omics approaches may reveal underlying genetic and molecular pathways, supporting the development of targeted therapies. Additionally, post-vaccination optic neuritis requires further investigation to distinguish it from infection-related cases. Long-term follow-up is essential to assess recurrence risk and address current gaps caused by retrospective designs and inconsistent serological testing. By presenting a combined immune-vascular pathogenic model, this report highlights a potential distinct subtype of optic neuritis and provides a framework for improved diagnostics and mechanism-based therapies.
Conclusions
COVID-19 can trigger optic neuritis, and clinicians should remain vigilant. Patients presenting with sudden vision loss require prompt immunological and imaging studies to confirm the diagnosis. Early steroid pulse therapy significantly improves outcomes. The condition likely results from a combination of direct viral invasion, immune hyperactivation, and vascular dysfunction. This case proposes a potential pathogenic model, highlights a possible new subtype of optic neuritis, and suggests new diagnostic and therapeutic approaches, laying the groundwork for future clinical advances. As COVID-19 management strategies evolve, monitoring post-vaccination neurological complications remains essential. Future research should integrate clinical and molecular data to clarify underlying mechanism and guide targeted therapies.
List of abbreviations
DON, demyelinating optic neuritis
IDON, idiopathic demyelinating optic neuritis
MS-ON, multiple sclerosis-related optic neuritis
NMOSD-ON, neuromyelitis optica spectrum disorder-related optic neuritis
MOG-ON, MOG antibody-associated optic neuritis
CRION, chronic relapsing inflammatory optic neuropathy
RNFL, retinal nerve fiber layer
GCL, ganglion cell layer
IVMP, intravenous methylprednisolone
Correction notice
None
Acknowledgements
None
Author Contributions
(I) Conception and design: Shujuan Li, Yue Fu, Hui Yang
(II) Administrative support: Hui Yang
(III) Provision of study materials or patients: Yue Fu, Hui Yang
(IV) Collection and assembly of data: Shujuan Liu
(V) Data analysis and interpretation: Shujuan Liu, Yue Fu
(VI) Manuscript writing: All authors
(VII) Final approval of manuscript: All authors
Conflict of Interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form.
Patient consent for publication
None
Ethics approval and consent to participate
None
Data availability statement
None
Open access
This is an Open Access article distributed inaccordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication anddistribution of the article with the strict proviso that no changes or edits are made and the original work isproperly cited (including links to both the formalpublication through the relevant DOI and the license).