(A) Visual acuity HM of the right eye, central corneal ulcer about 6 mm, feathery edge, moss formation. (B) 2 days after surgery, visual acuity HM, implant edema, no interlaminar effusion, bubble injection during anterior chamber partially absorbed. Tacrolimus eye fluid, bromfenac sodium eye fluid, sodium hyaluronate eye fluid, itraconazole 0.2 g, once a day, for 3 weeks. (C, D) 10 days after surgery, visual acuity was counting fingers (CF), edema was relieved, the epithelium was repaired, and there was no interlaminar effusion. The treatment was continued as before. (E) One month after surgery, visual acuity was 3.7, transparency was good, and no loosening of sutures was observed. 5:30 o’clock location of the limbus cornea Limbal neovascularization invades intercorneal layer. Stop bromfenac sodium eye fluid, add loteprednol eye fluid. (F) 3 months after surgery, visual acuity was 4.0 and corrected visual acuity was 4.4. The central area of the implant was transparent and some sutures were removed. The pupil is 3 mm in diameter and slightly insensitive to light reflex. Remove all sutures and continue anti-rejection therapy. (G) 18 months after surgery, visual acuity was 4.5 and corrected visual acuity was
4.7. The pupil area implant has good transparency. 5:30 o’clock location of the limbus cornea, the neovascularization became thinner and some atrophy. Continue tacrolimus eye fluid, 2 times per day.
Figure 3 Case 3: The patient is a 67-year-old male, with the left eye eyesight decline in 2 d, pseudomonas aeruginosa ulcer, biological engineering corneal andante layer corneal transplantation, postoperative systemic intravenous drip 3 days amikacin therapy, local tobramycin eye drops 1 time per hour, tacrolimus eyedrops eye 4 times per day, bromfenac sodium eye drops eye for 2 times per day, the sodium hyaluronate drops eye 4 times per day
(A) Preoperative vision HM, the conjunctiva of the left eye was highly hyperemic and edema, the gray and white ulcerated surface of the central cornea was about 6 mm in diameter, the matrix was dissolved and thin, and purulent secretions were attached. (B) 3 days after the operation, the visual acuity was CF, the implant was gray and white with edema, and no interlayer effffusion was observed. Continue treatment as before. (C, D) 14 days after surgery, visual acuity was 4.1, the graft was transparent, and the epithelium was well repaired. The sutures did not come loose. Antibiotics were stopped and anti-rejection therapy continued. (E) 1 month after surgery, visual acuity was 4.2, corrected visual acuity was 4.5, and no loosening of sutures was observed. Continue anti-rejection therapy. (F) 3 months after surgery, visual acuity was 4.2, corrected visual acuity was 4.5, and no loosening of sutures was observed. The sutures were removed and anti-rejection therapy continued. (G) 14 months after surgery, visual acuity was 4.4 and corrected visual acuity was 4.6. The phytophilic margin is pale and slightly cloudy. Tacrolimus eye drops were recommended for 2 times per day and outpatient follow-up.
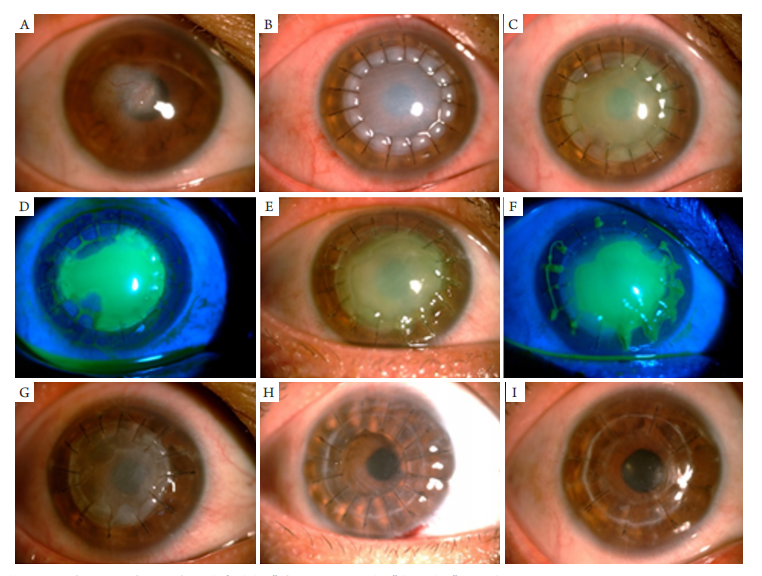
图4 病例4:患者女,39岁,行右眼病毒性角膜炎行生物工程角膜板层角膜移植术
Figure 4 Case 4: A 39-year-old female patient with right eye viral keratitis underwent bioengineered lamellar keratoplasty
(A) Preoperative visual acuity was CF, and the diameter of the corneal pupil area was about 3.5 mm. (B) 2 days after the operation, the visual acuity was HM, the implant was gray and white with edema, and no interlayer effffusion was observed. Tacrolimus eye infusion 4 times per day, prednisolone eye infusion 2 times per day, sodium hyaluronate eye infusion 4 times per day. (C, D) 10 days after surgery, the visual acuity was CF, the graft edema was reduced, and most of the epithelium was not repaired. The sutures did not come loose. Calf serum eye gel was applied 4 times per day. (E, F) 1 month after surgery, visual acuity HM, extensive loss of graft epithelium, partial dissolution and thinning of matrix. Remove loose sutures and resuture. The treatment is the same. (G) 2 months after surgery, the visual acuity was CF, no loosening of the suture was observed, the graft epithelium was repaired, the matrix was partially dissolved and thinned, and gray pall was formed. Bioengineered corneal grafts were removed and allogeneic human grafts replaced. Continue anti-rejection therapy. (H) One month after the second operation, visual acuity was 4.2 and corrected visual acuity was 4.4. Continue anti-rejection therapy. (I) 3 months after the second operation, visual acuity was 4.5 and corrected visual acuity was 4.8. The graft was transparent and some sutures were removed.
开放获取声明 本 文 适 用 于 知 识 共 享 许 可 协 议( C r e a t i v e Commons),允许第三方用户按照署名(BY)-非商业 性使用(NC)-禁止演绎(ND)(CC BY-NC-ND)的方式共 享,即允许第三方对本刊发表的文章进行复制、发 行、展览、表演、放映、广播或通过信息网络向公众 传播,但在这些过程中必须保留作者署名、仅限于 非商业性目的、不得进行演绎创作。详情请访问: https://creativecommons.org/licenses/by-nc-nd/4.0/。
1. Xiao YT, Zhao XY, Liu X, et al. Ten-year follow-up of lamellar keratoplasty treatment with acellular porcine corneal stroma: a case report[ J]. Cornea, 2022, 41(5): 623-626.
2. Li S, Li M, Gu L, et al. Risk factors influencing survival of acellular porcine corneal stroma in infectious keratitis: a prospective clinical study[ J]. J Transl Med, 2019, 17(1): 434.
3. Zhang Y, Hu Z, Qu J, et al. Tissue-engineered corneal endothelial sheets using ultrathin acellular porcine corneal stroma substrates for endothelial keratoplasty[ J]. ACS Biomater Sci Eng, 2022, 8(3): 1301-1311.
4. Li S, Xiao P, Deng Y, et al. Acellular porcine corneal stroma may not be optimal for peripheral keratoplasty: reports of 2 cases[ J]. Cornea, 2021, 40(4): 502-505.
5. Zhang K, Ren XX, Li P, et al. Construction of a full-thickness human corneal substitute from anterior acellular porcine corneal matrix and human corneal cells[ J]. Int J Ophthalmol, 2019, 12(3): 351-362.
6. Li H, Dong M, Zhou Q, et al. Corneal calcification of acellular porcine corneal stroma following lamellar keratoplasty[ J]. Acta Ophthalmol, 2022, 100(2): 164-174.
7. 程燕, 吴洁, 朱海峰, 等. 生物工程角膜移植术后排斥反应的临床及免疫病理观察: 附5例报告[ J]. 国际眼科杂志. 2021, 21(9): 1661-1664.
CHENG Yan , WU Jie, ZHU Haifeng , etal . Clinical and immunopathological study of rejection after bioengineered keratoplasty: a report of 5 cases[ J]. International Eye Science, 2021, 21(9): 1661-1664.
8. Li H, Zhao L, Wang F, et al. Natural cross-linker-stabilized acellular porcine corneal stroma for lamellar keratoplasty[ J]. Acta Biomater, 2020, 114: 270-284.
9. 段虎成, 陈瑞, 罗嘉婧. 猪脱细胞角膜基质人板层角膜移植术后植片上皮化的临床观察[ J]. 眼科学报, 2019, 34(2): 85-89.
DUAN Hucheng, CHEN Rui, LUO Jiajing. Clinical observation of the epithelization of grafts after human lamellar keratoplasty with acellular porcine corneal stroma[ J]. Eye Science, 2019, 34(2): 85-89.
10. Li S, Deng Y, Tian B, et al. Healing characteristics of acellular porcine corneal stroma following therapeutic keratoplasty[ J]. Xenotransplantation, 2020, 27(2): e12566.
11. Zheng Q, Zhang Y, Ren Y, et al. Deep anterior lamellar keratoplasty with cross-linked acellular porcine corneal stroma to manage fungal keratitis[ J]. Xenotransplantation, 2021, 28(2): e12655.
12. Chen Y, Zhang L, Liu Z, et al. Efficacy of lamellar keratoplasty with acellular porcine corneal stroma in treatment for infectious central and peripheral corneal ulcers[ J]. Ther Clin Risk Manag, 2021, 17: 623-634.
13. Zheng J, Huang X, Zhang Y, et al. Short-term results of acellular porcine corneal stroma keratoplasty for herpes simplex keratitis[ J]. Xenotransplantation, 2019, 26(4): e12509.
14. 范祥雨, 黄霏霏, 张朝然, 等. 利用猪角膜脱细胞基质行板层角膜移植手术治疗感染性 角膜炎的临床研究[ J]. 中国眼耳鼻喉科杂志, 2021, 21(5): 330-334.
FAN Xiangyu, HUANG Feifei, ZHANG Chaoran et al. Clinical study on the treatment of infectious keratitis with lamellar keratoplasty using porcine corneal acellular stroma[ J]. Chinese Journal of Ophthalmology and Otorhinolaryngology, 2021, 21(5): 330-334.
15. 曲晓瑜, 储昭节, 马强, 等. 生物工程角膜移植治疗病毒性角膜炎疗效观察[ J]. 海南医学, 2019, 30(21): 2805-2807.
QU Xiaoyu, CHU Zhaojie, MA Qiang, et al. Effect of bioengineered corneal transplant for treatment of herpes simplex keratitis[ J]. Hainan Medical Journal, 2019, 30(21): 2805-2807.
16. 林莉. 生物工程角膜移植治疗感染性角膜炎[ J]. 国际眼科杂志, 2019, 19(10): 1728-1732.
LIN Li. Bioengineered keratoplasty for infectious keratitis[ J]. International Eye Science, 2019, 19(10): 1728-1732.
17. 刘全坤, 李恒, 杨旭苟, 等. 生物工程角膜移植对真菌性角膜溃疡的临床疗效及其对组 织形态学的影响[ J]. 中国医学前沿杂志(电子版), 2021, 13(11): 102-106.
LIU Quankun, LI Heng, YANG Xugou, et al. The clinical effect of bioengineered corneal transplantation on fungal corneal ulcer and its influence on histomorphology[ J]. Chinese Journal of the Frontiers of Medical Science. Electronic Version, 2021, 13(11): 102-106.
18. 史伟云. 以生物工程角膜为供体的板层角膜移植术治疗真菌性角膜炎[ J]. 中华眼科杂志, 2019, 55(6): 463.
SHI Weiyun. Lamellar keratoplasty with bioengineering cornea as donor in the treatment of fungal keratitis[ J]. Chinese Journal of Ophthalmology, 2019, 55(6): 463.
19. 刘志玲, 高明宏, 陈颖欣. 生物工程角膜与人供体角膜治疗真菌性角膜溃疡的比较[J]. 中国组织工程研究, 2020, 24(10): 1563-1569.
LIU Zhiling, GAO Minghong, CHEN Yingxin. Bio-engineering cornea versus human donor cornea in the treatment of fungal corneal ulcer[ J]. Chinese Journal of Tissue Engineering Research, 2020, 24(10): 1563-1569.
20. 史伟云, 高华. 中国角膜病诊疗技术70年发展回顾[ J]. 中华眼科杂志, 2020, 56(6): 401-408.
SHI Weiyun, GAO Hua. A summar y of China’s 70 years of development in diagnosis and treatment targeting corneal diseases[ J].Chinese Journal of Ophthalmology, 2020, 56(6): 401-408.
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)