(A) Prior to each block of binocular rivalry task, participants adjusted the position of dichoptic images of the frames and fixation crosses to ensure binocular fusion. After that, two orthogonal gratings were presented to the two eyes dichoptically. Participants viewed the dichoptic images for 60 s and reported their dominant percept using keyboard. After 10 s for resting, the next trial was initiated. (B) Participants first performed the binocular rivalry task to obtain the baseline of binocular balance, and then performed the peripheral patching of one eye for 90 min, and subsequently completed the binocular rivalry tasks at each timepoint, to evaluate the changes in binocular dominance over time.
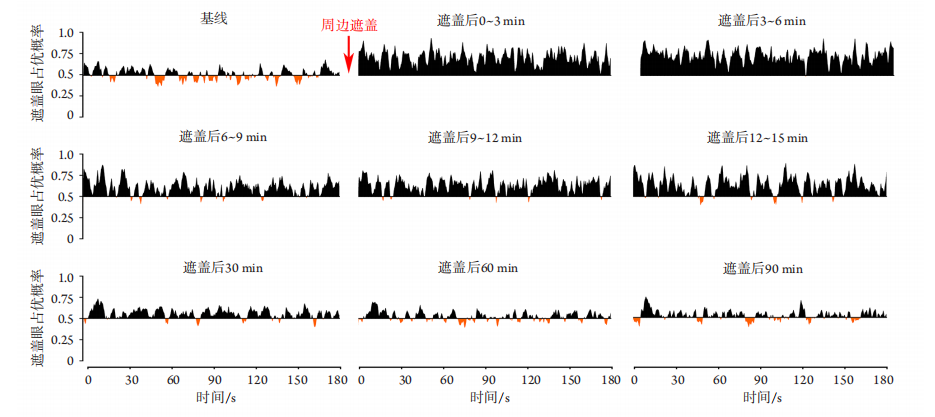
Figure 2 Changes in the average proportion of times participants reported seeing the stimulus presented to the patched eye before and after peripheral patching
在基线处,水平轴(X轴)上下方曲线数量和曲线下面积基本相等,即对被遮盖眼的应答概率与随机概率相近,提示双眼基 本平衡。周边遮盖后,X轴上方曲线下面积明显增加,提示受试者更有可能看到呈现在被遮盖眼的视觉刺激。60、90 min 时双眼基本恢复平衡。X轴以上代表被遮盖眼占优,X轴以下代表非遮盖眼占优。
At the baseline, the number of curves and the area under curve (AUC) above and below the X-axis were basically similar, indicated that the probability of reporting the stimuli presented to the patched eye was similar to the random probability, so the dominance of the two eyes were balanced. After the removal of peripheral patching, the number of curves and the AUC above the X-axis increased significantly, suggesting that participants were more likely to report the stimuli presented to the patched eye. The dominance of the two eyes did not rebalance until post-60 min. Curves above the X-axis represents the predominance of the patched eye, while those below the X-axis represents the predominance of the non-patched eye.
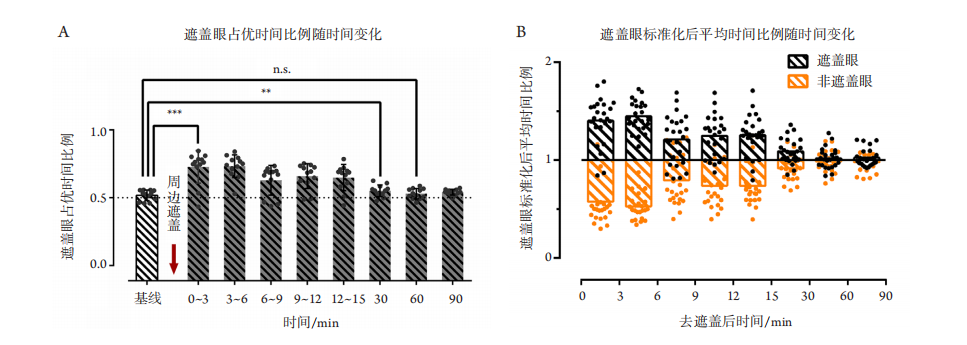
进一步通过单因素重复测量ANOVA分析不同时间段间遮盖眼占优时间的改变(图3 ),经箱线图判断,数据无异常值;经Shapiro-Wilk检验,各组数据服从正态分布(P>0.05);经过Mauchly’s
球形假设检验,因变量的方差协方差矩阵不相等,χ 2
(35)=84.517,P<0.001,通过Greenhouse &
Geisser方法校正ε =0.576。去遮盖前后各时间段间(基线、0~3 min、3~6 min 、6~9 min、
9~12 min 、 12~15 min 、30 min 、60 min 、90 min)发生显著改变[校正后F(4.607,105.95)=28.211,P<0.001,偏ω2
=0.502]。通过事后LSD-t检验可发现直至去遮盖后的30 min,遮盖眼的占优时间仍显著高于基线(基线 vs 0~3 min,基线 vs 3~6 min,
基线 vs 6~9 min,基线 vs 9~12 min,基线 vs 12~
15 min,均P<0.001;基线 vs 30 min,P=0.002,小于多重检验校正后的P值(0.05/8=0.006),提示周边遮盖显著改变了中央视觉的双眼优势平衡,且使双眼平衡向被遮盖眼倾斜。随着去遮盖后的时间延长,遮盖眼的占优时间逐渐减少,60、90 min与基线差异均无统计学意义(基线 vs 60 min,P=0.445;基线 vs 90 min,P=0.196)。
(A) The proportion of the patched eye dominance durations at 0–3 min, 3–6 min, 6–9 min, 9–12 min, 12–15 min and 30 min after the removal of the patch were significantly higher than the baseline. Neither the proportion of the patched eye dominance duration at the 60 min nor that at 90 min was significantly different from the baseline. B. The normalized mean dominance duration for each eye (the ratio of dominance duration at each timepoint to that at baseline) after the removal of patch. The ratio of 1 means that the dominance duration is similar to the baseline, while the ratio more or less than 1 means that the dominance duration is above or below the baseline, respectively. Until 30 min after the removal of peripheral patching, the dominance duration of the patched eye increased significantly, while the corresponding non-patched eye dominance duration decreased. At 60 min, the dominance duration of each eye basically returned to the baseline level.
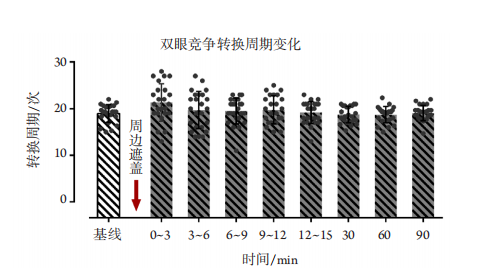
各时间段的眼优势转换周期变化如图4所示。
单因素重复测量ANOVA未发现各时间段间转换周期差异有统计学意义[校正F(5.227,120.225)=2.127,
P =0.064,偏ω2
=0.040]。尽管未发现各时间段间的眼优势转换周期差异,配对t检验发现去遮盖后的3 min内转换周期显著大于基线(P =0.020),
而其余时间段间差异均无统计学意义 ( 基 线 v s
3~6 min,基线 vs 6~9 min,基线 vs 9~12 min,
基 线 vs 12~15 min,基线 vs 30 min,基线 vs
60 min,基线 vs 90 min,均P>0.05)。 同一受试者均在不同时间 (间隔1周) 完成了主导眼和非主导眼的单眼周边遮盖。分别对主导/非主导眼进行单因素重复测量ANOVA分析发现,不论是遮盖主导眼 [ F(8,88)=13.067 ,
P < 0.001 , 偏 ω 2
=0.472] ,还是遮盖非主导眼[校正后F(3.76,41.363)=14.676 ,P < 0.001 ,偏
ω2
=0.503],遮盖眼占优时间比例均发生显著改变。但通过事后 LSD- t 检验发现,遮盖主导眼在30 min的遮盖眼占优时间比例与基线差异无统计学意义(基线 vs 30 min,P =0.132); 除6 ~
9 min(P=0.008,多重比较校正大于多重检验校正后的P值(0.05/8=0.006)外,0~3 min(P<0.001)、
3~6 min( P < 0.001) 、 9~12 min( P < 0.001) 、
12~15 min( P < 0.001) 仍显著高于基线。除
6~9 min(P=0.037)和9~12 min(P=0.009)外,遮盖非主导眼所引起的遮盖眼占优时间比例在30 min
内的各时间段与基线比较,差异均有统计学意义(基线 vs 0~3 min,P<0.001;基线 vs 3~6 min,
P<0.001;基线 vs 12~15 min,P=0.001;基线 vs
30 min,P=0.004,多重比较校正小于多重检验校正后的P值(0.05/8=0.006)。进一步比较去遮盖后的0~3 min遮盖眼占优时间比例相对基线的改变幅度,发现遮盖主导眼引起的占优时间比例改变
幅度与遮盖非主导眼间差异无统计学意义(配 对
t 11=0.214,P=0.835)
图4 双眼竞争转换周期变化图示:周边遮盖前后双眼竞争转换周期无显著改变
Figure 4 Dominance switch between the two eyes shows that there was no significant change in the dominance switch among baseline and each timepoint after peripheral patching
1. 广东省自然科学基金 (2015A030312016);广东省基础与应用基础研究基金 (2021A1515110479)。This work was supported by the Natural Science Foundation of GuangdongProvince (2015A030312016) and the Guangdong Basic and Applied Basic Research Foundation (2021A1515110479), China
参考文献
1. Hussain Z, Webb BS, Astle AT, et al. Perceptual learning reduces crowding in amblyopia and in the normal periphery[ J]. J Neurosci,2012, 32(2): 474-480.
2. Lunghi C, Sframeli AT, Lepri A, et al. A new counterintuitive training for adult amblyopia[ J]. Ann Clin Transl Neurol, 2019, 6(2): 274-284.
3. Mitchell DE, Maurer D. Critical periods in vision revisited[ J]. Annu Rev Vis Sci, 2022, Epub ahead of print. doi:10.1146/annurev-vision-090721-110411.
4. Consorti A, Sansevero G, Torelli C, et al. Visual perceptual learning induces long-lasting recovery of visual acuity, visual depth perception abilities and binocular matching in adult amblyopic rats[ J]. Front Cell Neurosci, 2022, 16: 840708.
5. Stewart CE, Moseley MJ, Stephens DA, et al. Treatment dose-response in amblyopia therapy: the Monitored Occlusion Treatment of Amblyopia Study (MOTAS)[ J]. Invest Ophthalmol Vis Sci, 2004,45(9): 3048-3054.
6. Birch EE, Stager DR . Long-term motor and sensory outcomes after early surgery for infantile esotropia[ J]. J AAPOS, 2006,10(5): 409-413.
7. Meier K , Tarczy-Hornoch K . Recent treatment advances in amblyopia[ J]. Annu Rev Vis Sci, 2022, Epub ahead of print. doi:
10.1146/annurev-vision-100720-022550.
9. Wiesel TN, Hubel DH. Comparison of the effects of unilateral and bilateral eye closure on cortical unit responses in kittens[ J]. J Neurophysiol, 1965, 28(6): 1029-1040.
10. Kiorpes L, Daw N. Cortical correlates of amblyopia[ J]. Vis Neurosci,2018, 35: E016.
11. Knapen T, Brascamp J, Adams WJ, et al. The spatial scale of perceptual memory in ambiguous figure perception[ J]. J Vis, 2009, 9(13): 1-12.
12. Zhao W, Jia WL, Chen G, et al. A complete investigation of monocular and binocular functions in clinically treated amblyopia[ J]. Sci Rep,2017, 7(1): 10682.
13. Rice ML, Leske DA, Smestad CE, et al. Results of ocular dominance testing depend on assessment method[ J]. J AAPOS, 2008, 12(4):365-369.
14. Liu ZT, Chen ZD, Gao L, et al. A new dichoptic training strategy leads to better cooperation between the two eyes in amblyopia[ J]. Front Neurosci, 2020, 14: 593119.
15. Smith EL, Ramamirtham R, Qiao-Grider Y, et al. Effects of foveal ablation on emmetropization and form-deprivation myopia[ J]. Invest Ophthalmol Vis Sci, 2007, 48(9): 3914-3922.
16. Zurevinsky J. Eccentric fixation and inverse occlusion: renewing our interest?[ J]. J Binocul Vis Ocul Motil, 2019, 69(4): 136-140.
17. Lunghi C, Burr DC, Morrone C. Brief periods of monocular deprivation disrupt ocular balance in human adult visual cortex[ J]. Curr Biol, 2011,21(14): R538-R539.
18. Zhou JW, He ZF, Wu YD, et al. Inverse occlusion: a binocularly motivated treatment for amblyopia[ J]. Neural Plast, 2019, 2019:
5157628.
19. Zhou JW, Baker DH, Simard M, et al. Short-term monocular patching boosts the patched eye's response in visual cortex[ J]. Restor Neurol Neurosci, 2015, 33(3): 381-387.
20. Holmes JM, Levi DM. Treatment of amblyopia as a function of age[ J]. Vis Neurosci, 2018, 35: E015.
21. Li TJ, Qureshi R , Taylor K . Conventional occlusion versus pharmacologic penalization for amblyopia[ J]. Cochrane Database Syst Rev, 2019, 8(8): CD006460.
22. Wang S, Wen W, Zhu WQ, et al. Effect of combined atropine and patching vs patching alone for treatment of severe amblyopia in children aged 3 to 12 years a randomized clinical trial[ J]. JAMA Ophthalmol,2021, 139(9): 990-996.
23. Wallace DK, Lazar EL, Holmes JM, et al. A randomized trial of increasing patching for amblyopia[ J]. Ophthalmology, 2013, 120(11):2270-2277.
24. Holmes JM, Kraker RT, Beck RW, et al. A randomized trial of prescribed patching regimens for treatment of severe amblyopia in children[ J]. Ophthalmology, 2003, 110(11): 2075-2087.
25. Holmes JM, Repka MX , Kraker RT, et al. The treatment of amblyopia[ J]. Strabismus, 2006, 14(1): 37-42.
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)