Surgically induced scleral staphyloma
阅读量:1568
DOI:doi: 10.3978/j.issn.1000-4432.2017.03.03
发布日期:2024-12-29
作者:
Yong Yao
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Scleral staphyloma
corneal dermoid
cataract
pterygium
scleral patch graft
摘要
Background: To report the clinical features of surgically induced scleral staphyloma and investigate the
management.
Methods: Retrospective uncontrolled study.
Results: A full ophthalmological evaluation of surgically induced scleral staphyloma in four patients
was performed. The first patient was a 3-year-old young girl underwent corneal dermoid resection. The
second patient was a 60-year-old man underwent nasal pterygium excision and conjunctival autograft
without Mitomycin C (MMC). The other two were respectively a 74-year-old woman and a 69-year-old
man underwent cataract surgery. All patients performed allogeneic sclera patch graft. In the at least half
a year follow-up, the best corrected visual acuity (BCVA) of all the four patients were no worse than that
of preoperative. Ocular symptoms disappeared, including eye pain, foreign body sensation, and so on.
Unfortunately, the fourth patient showed sclera rejection and partial dissolution at postoperative 1 month.
Conclusions: Surgically induced scleral staphyloma must be considered in the differential diagnosis of
patients with staphyloma following corneal dermoid, pterygium, and cataract surgery. Allogeneic sclera patch
graft is one of the methods for treating scleral staphyloma. However sclera rejection and dissolution should
be considered postoperatively.
全文
Introduction
Common reasons for staphyloma formation include
surgery, trauma, inflammation, glaucoma, high myopia,
malnutrition, and developmental abnormalities. Surgically
induced scleral staphyloma had been reported in cataract
surgery, pterygium surgery, and so on (1,2). We report
several cases of sclera staphyloma induced by surgery,
involving corneal dermoid resection, cataract surgery,
and pterygium surgery, with descriptions and treatment
that may help surgeons to further manage those special
situations.
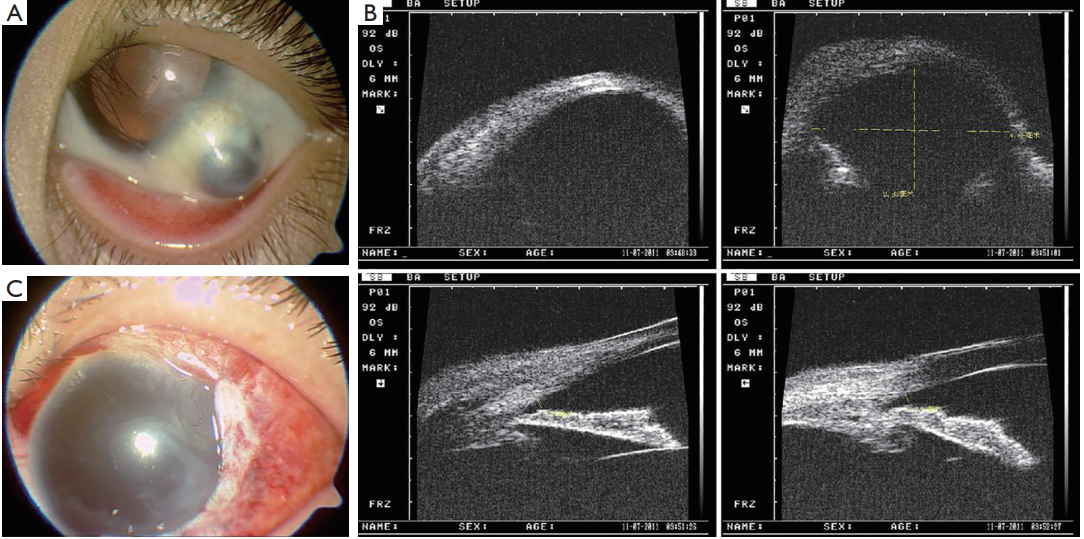
Case 1 (Figure 1): a 3-year-old young girl was referred to our hospital with a history of congenital corneal dermoid resection without graft one year ago. She complained of foreign body sensation and “black lump” on the operated eye postoperatively. No other history was reported. Best-corrected visual acuity (BCVA) was 4/20 in the left eye and intraocular pressure (IOP) was 15 mmHg. Slit-lamp examination revealed a 6 mm × 7 mm brown protruding bulge on the infratemporal. The anterior chamber and fundus examination showed no abnormal. BCVA was 12/20 and slit-lamp examination showed no obvious abnormalities in the right eye. Laboratory examinations results were normal, including blood-R, urine-R, blood biochemistry, hemostatic, HIV, HCV, HBSAg, RPR, chest X-ray, electrocardiogram and other immune inspections. The diagnosis of Scleral staphyloma was given and an operation of Sclera patch graft was performed. In the period of 30 months following-up, the BCVA was 10/20 and the foreign body sensation disappeared in the left eye. Slit-lamp examination revealed no scleral rejection and conjunctival dissolution.
Materials and results
All patients were referred to Joint international eye center
of Shantou University and The Chinese University of
Hong Kong. Surgical methods were scleral patch graft,
combined autologous conjunctival pedicle transposition at
the same time if necessary. Allogeneic scleras, which were
glycerol cryopreservation, were provided by the eye bank
of Joint international eye center of Shantou University and
The Chinese University of Hong Kong. The minimum
age of the patient was 3 years old, and the maximum was
74 years old. The average age was 50 years old. Three
patients were female and one was male. They had a
surgery history of corneal dermoid, cataract, pterygium,
respectively. All patients provided informed consent, and
this study adhered to the tenets of the Declaration of
Helsinki [Ethic Approval ID: EC 20160616(4)-A12]. The
following was medical records: Case 1 (Figure 1): a 3-year-old young girl was referred to our hospital with a history of congenital corneal dermoid resection without graft one year ago. She complained of foreign body sensation and “black lump” on the operated eye postoperatively. No other history was reported. Best-corrected visual acuity (BCVA) was 4/20 in the left eye and intraocular pressure (IOP) was 15 mmHg. Slit-lamp examination revealed a 6 mm × 7 mm brown protruding bulge on the infratemporal. The anterior chamber and fundus examination showed no abnormal. BCVA was 12/20 and slit-lamp examination showed no obvious abnormalities in the right eye. Laboratory examinations results were normal, including blood-R, urine-R, blood biochemistry, hemostatic, HIV, HCV, HBSAg, RPR, chest X-ray, electrocardiogram and other immune inspections. The diagnosis of Scleral staphyloma was given and an operation of Sclera patch graft was performed. In the period of 30 months following-up, the BCVA was 10/20 and the foreign body sensation disappeared in the left eye. Slit-lamp examination revealed no scleral rejection and conjunctival dissolution.
Figure 1 Scleral staphyloma after corneal dermoid resection. (A) Pre-op; (B) UBM pre-op; (C) post-op. UBM, ultrasound biomicroscopy.
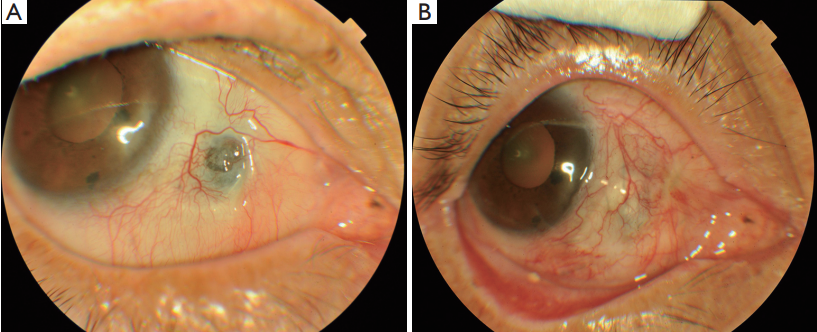
Case 2 (Figure 2): a 60-year-old woman was admitted in our
hospital with a history of pterygium excision and conjunctival
autograft without MMC in the right eye at local hospital
5 years ago. No history of systemic or other ocular diseases was
reported. She complained of foreign body sensation and prick
pain on the operational eye 2 weeks post operatively, which
could not be alleviated by local artificial tears, corticosteroid
hormone eye drops, nonsteroidal anti-inflammatory
drug, tacrolimus eye drops, and autologous serum eye
drops. BCVA was 12/20 in the right eye and IOP was
14 mmHg. Slit-lamp examination revealed a 2 mm × 3 mm
scleral partial dissolution and local conjunctiva was
dissolved. Corneal fluorescein staining showed negative
and Tear break-up time was 9 seconds in the cornea. Other
examination showed no abnormality. BCVA was 16/20
and clinical examination showed no obvious abnormalities
in the left eye. Laboratory examinations results were
normal, including blood-R, urine-R, blood biochemistry,
hemostatic, HIV, HCV, HBSAg, RPR, chest X-ray,
electrocardiogram and other immune inspection. The
diagnosis of scleral staphyloma after pterygium surgery was
given and an operation of scleral patch graft and autologous
conjunctival pedicle transposition were performed. Topical
corticosteroids, immunosuppressants, artificial tears
continued for 3 months. In the period of 24 months follow-up, the BCVA was 12/20 and the symptoms disappeared
in the right eye. Slit-lamp examination revealed no scleral
rejection and conjunctival dissolution.
Figure 2 Scleral staphyloma after pterygium excision and conjunctival autograft without MMC. (A) Pre-op; (B) post-op. MMC, Mitomycin C.
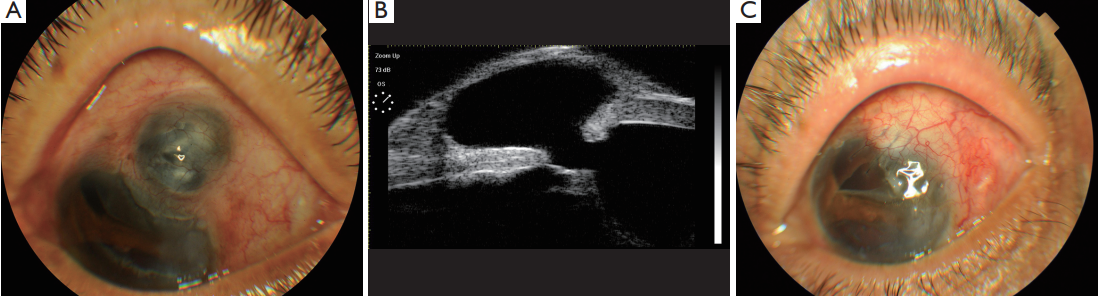
Case 3 (Figure 3): a 63-year-old man was referred to
our hospital with a history of explosive injury and cataract
surgery at local hospital in the left eye 20 years ago. No
other history was reported except cerebral thrombosis
and hypertension for ffve years. He had complained of red
eye, pain, foreign body sensation, symptoms increase for
1 year. BCVA was hand movement in the left eye and IOP
was 12 mmHg. Slit-lamp examination revealed a 6 mm ×
6 mm brown protruding bulge on the superior temporal
limbus. The cornea was opacity (+), and the anterior
chamber depth is normal. There was iridodialysis from 4:00
to 9:00 clock, and the pupil was irregular and crystal was
absent. Fundus examination showed no abnormality. The
BCVA was 16/20 and clinic examination showed no obvious
abnormalities in the right eye. Laboratory examination
results were normal, including blood-R, urine-R, blood
biochemistry, hemostatic, HIV, HCV, HBSAg, RPR, chest
X-ray, electrocardiogram and other immune inspection. The
diagnosis was obviously of left eye: (I) scleral staphyloma;
(II) iridodialysis; (III) aphakia; (IV) obsolete explosive
injury. The operation of scleral patch graft and autologous
conjunctival pedicle transposition were performed .In the 9
months follow-up, BCVA was hand movement, scleral graft
was in position and conjunctival ffap completely covered the
sclera without dissolution.
Figure 3 Scleral staphyloma after traumatic cataract surgery. (A) Pre-op; (B) UBM pre-op; (C) post-op. UBM, ultrasound biomicroscopy.
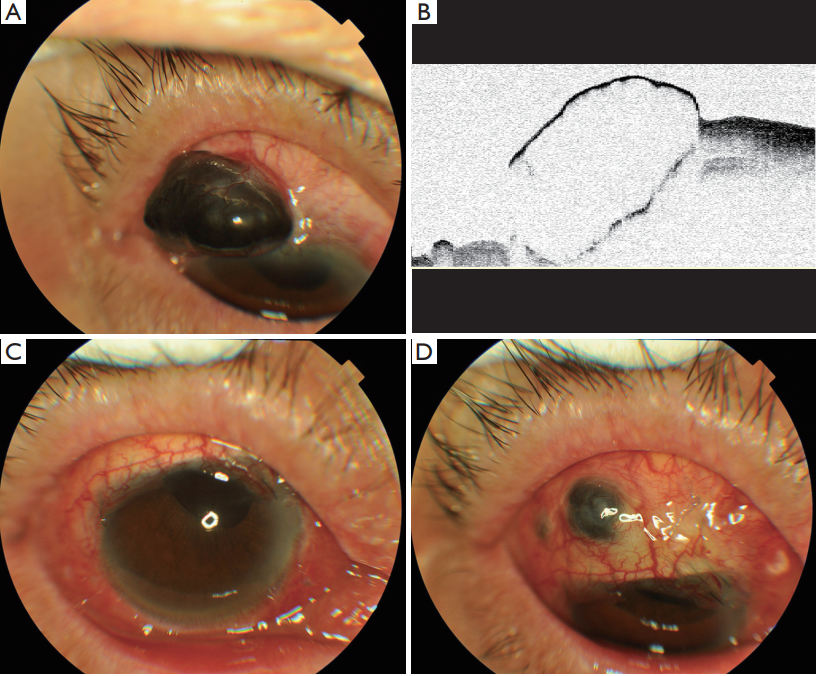
Case 4 (Figure 4): a 74-year-old woman was admitted
to our hospital with a history of cataract surgery at local
hospital in the right eye 12 years ago. She had neither
systemic history nor other ocular disease except eyeball
atrophy in the left eye, because of standing retinal
detachment. She had complained of a black bulging material
which gradually increases in the right eye postoperatively.
She did not come to a doctor because of money until she
suffered from obvious eye pain and foreign body sensation
for 1 year. BCVA was hand movement in the right eye and IOP was 12 mmHg. Slit-lamp examination revealed a
6 mm × 10 mm brown protruding bulge on the superior
temporal. The pupil shift upward and the crystal were
absent. Fundus examination showed no abnormality. BCVA
was no light perception, and slit-lamp examination showed
corneal leucoma and eyeball atrophy in the left eye. The
anterior segment OCT of right eye showed: Line-like bulge
strong reflection, and underneath was cystic, showed low
internal reffection area. Laboratory examination results were
normal, including blood-R, urine-R, blood biochemistry,
hemostatic, HIV, HCV, HBSAg, RPR, chest X-ray,
electrocardiogram and other immune inspection. The
diagnosis of scleral staphyloma and aphakia was given of
right eye. The operation of scleral patch graft and autologous
conjunctival pedicle transposition was performed. In the
half year of follow-up, BCVA was hand movies, eye pain and
foreign body sensation alleviate. Unfortunately, she showed
scleral rejection and partial dissolution (2 mm × 2 mm)
1 month postoperatively. Topical corticosteroids lasted
for 1 month taking into account that the corticosteroids
may cause sclera dissolution aggravate, and Topical
immunosuppressants, artificial tears continued. We suggest
the contralateral eye autologous sclera patch graft if necessary
but it was not accepted by the patient’s family. No further
treatment was accepted except local eye drops. Fortunately,
scleral dissolution presented no further aggravation, and
the patients had no foreign body sensation, pain, or other
symptoms. This patient is still in follow-up now.
Figure 4 Scleral staphyloma after cataract surgery. (A) Pre-op; (B) anterior segment optical coherence tomography (AS-OCT) pre-op; (C)
post-op; (D) 1 month post-op.
Discussion
Anatomically corneal dermoids have been classified into
three grades: Grade I limbal or epibulbar dermoid are
lesions with a superffcial tumor measuring less than 5 mm.
Grade II limbal dermoids are of larger size and extend into
the corneal stroma down to Descemet’s membrane. Grade
III limbal dermoids involve the whole cornea and structures
of the anterior chamber. Visual acuity may be reduced due
to the presence of coexisting amblyopia, astigmatism, and
obscuration of the visual axis by the tumor. Irritation by the protruding cilia may also be a presenting feature. In the
past, several different surgical techniques for the removal
of dermoids have been described (3). These techniques
include bare excision, amniotic membrane transplantation,
and even lamellar and penetrating keratoplasty. The
adequate choice depends on the location and size of the
lesion. Major risks of the excision of the limbal dermoid are
intraoperative perforation, postoperative epithelial defects
and peripheral vascularization of the cornea (3). Lamellar
keratoplasty is reported to result in the improvement of
visual acuity, but may also lead to graft opaciffcation, graft
ectasia, corneal donor melt, and astigmatism (4,5). The
conventional method of treatment for dermoids is a simple
excision or a shaving operation. However, complications
including postoperative scars with neovascularization or
pseudopterygium have been frequently noted (6). The
prerequisite is superficial tumors and the remaining
corneoscleral is thick enough. In this 3-year-old young girl,
she presented scleral staphyloma 1 year after pterygium
surgery. We speculate that the main cause may be a thin
remaining sclera. In addition, the growth and development
of the eye cannot be ignored.
Pterygium excision with conjunctival autograft is a commonly performed procedure for the treatment of primary and recurrent pterygia. Scleral necrosis and melting can occur after pterygium surgery due to the use of adjunctive irradiation, mitomycin C, or excessive cauterization of the sclera (2). It is also believed to be a delayed-type hypersensitivity response to surgical trauma or ischemia that exposes tissue antigens, thereby sensitizing the immune system (7). In this case, no radiation or mitomycin C was used, and No systemic history was reported. The patient presented foreign body sensation and prick pain on the operational eye 2 weeks postoperatively. No evidence of infectious scleritis presented. We speculate that Sclera cauterization and ischemia may play an important role. It could not alleviate the symptoms after systemic medicine. An operation was strongly requested because local discomfort seriously affects her life.
Cataract surgery was another cause of sclera staphyloma, even though very rare. Sutured incision was malaligned and the top of the iris prolapsed, formed an incarceration. Although the IOP was low, the tissues including the sclera, choroid, or the iris protruded, expanding outward and ffnally forming a scleral staphyloma that resembled a purple black grape-shaped bulge, all secondary to postoperative damage to the eyeball wall that led to reduced resistance (1). This may be the main reason for the formation of the anterior scleral staphyloma in those patients. The cases we report has similar characteristics to that described by Zheng and associates (1) that showed formation of a ciliary staphyloma induced by a corneoscleral tunnel incision cracking following cataract surgery.
Zheng Q (1) reported successfully treat sclera staphyloma by combined anterior sclera staphylectomy and vitrectomy. The patient might present greater postoperative astigmatism. In addition, it might increase the chance of retinal detachment. Yalçindag (8) reported to repair sclera staphyloma with dehydrated dura mater patch graft. Ozcan (9) reported successfully treat scleral defects using fascia lata, cornea, and sclera as graft materials. However, both dura mater and fascia lata were not easy got in our hospital. Polat (10) reported successfully use of an autologous lamellar scleral graft to repair a scleral melt, but it was limited to a relatively small graft. All our patients were still slow progress, and Symptoms could not be relieved even after systemic medicine. The operation of Sclera patch graft was performed in all four patients, three of them combined autologous conjunctival pedicle transposition. In the at least half a year follow-up, the BCVA of all the four patients were no worse than that of preoperative. Ocular symptoms disappeared, including eye pain, foreign body sensation, and so on. Unfortunately, the fourth patient showed partial sclera dissolution 1 month postoperative. We speculate that the main cause may be sclera rejection and ischemia. Fortunately, scleral dissolution did not aggravate after the systemic use of postoperative topical corticosteroids, immunosuppressants and Chinese traditional medicine for systemic vasodilatory. Surgical intervention was not accepted and the patient is still in follow-up.
Our study has some limitations, including its retrospective design, the small number of patients, and the lack of a control group. Despite this, we can conclude that scleral staphyloma must be considered in the patients following corneal dermoid, pterygium, and cataract surgery, even rare. Allogeneic scleral patch is one of the methods for treating scleral staphyloma. However, scleral rejection and dissolution should be considered postoperatively.
Pterygium excision with conjunctival autograft is a commonly performed procedure for the treatment of primary and recurrent pterygia. Scleral necrosis and melting can occur after pterygium surgery due to the use of adjunctive irradiation, mitomycin C, or excessive cauterization of the sclera (2). It is also believed to be a delayed-type hypersensitivity response to surgical trauma or ischemia that exposes tissue antigens, thereby sensitizing the immune system (7). In this case, no radiation or mitomycin C was used, and No systemic history was reported. The patient presented foreign body sensation and prick pain on the operational eye 2 weeks postoperatively. No evidence of infectious scleritis presented. We speculate that Sclera cauterization and ischemia may play an important role. It could not alleviate the symptoms after systemic medicine. An operation was strongly requested because local discomfort seriously affects her life.
Cataract surgery was another cause of sclera staphyloma, even though very rare. Sutured incision was malaligned and the top of the iris prolapsed, formed an incarceration. Although the IOP was low, the tissues including the sclera, choroid, or the iris protruded, expanding outward and ffnally forming a scleral staphyloma that resembled a purple black grape-shaped bulge, all secondary to postoperative damage to the eyeball wall that led to reduced resistance (1). This may be the main reason for the formation of the anterior scleral staphyloma in those patients. The cases we report has similar characteristics to that described by Zheng and associates (1) that showed formation of a ciliary staphyloma induced by a corneoscleral tunnel incision cracking following cataract surgery.
Zheng Q (1) reported successfully treat sclera staphyloma by combined anterior sclera staphylectomy and vitrectomy. The patient might present greater postoperative astigmatism. In addition, it might increase the chance of retinal detachment. Yalçindag (8) reported to repair sclera staphyloma with dehydrated dura mater patch graft. Ozcan (9) reported successfully treat scleral defects using fascia lata, cornea, and sclera as graft materials. However, both dura mater and fascia lata were not easy got in our hospital. Polat (10) reported successfully use of an autologous lamellar scleral graft to repair a scleral melt, but it was limited to a relatively small graft. All our patients were still slow progress, and Symptoms could not be relieved even after systemic medicine. The operation of Sclera patch graft was performed in all four patients, three of them combined autologous conjunctival pedicle transposition. In the at least half a year follow-up, the BCVA of all the four patients were no worse than that of preoperative. Ocular symptoms disappeared, including eye pain, foreign body sensation, and so on. Unfortunately, the fourth patient showed partial sclera dissolution 1 month postoperative. We speculate that the main cause may be sclera rejection and ischemia. Fortunately, scleral dissolution did not aggravate after the systemic use of postoperative topical corticosteroids, immunosuppressants and Chinese traditional medicine for systemic vasodilatory. Surgical intervention was not accepted and the patient is still in follow-up.
Our study has some limitations, including its retrospective design, the small number of patients, and the lack of a control group. Despite this, we can conclude that scleral staphyloma must be considered in the patients following corneal dermoid, pterygium, and cataract surgery, even rare. Allogeneic scleral patch is one of the methods for treating scleral staphyloma. However, scleral rejection and dissolution should be considered postoperatively.
基金
暂无基金信息
参考文献
1. Zheng Q, Wu R, Li W. Combined anterior sclera staphylectomy and vitrectomy with anterior sclera staphyloma and vitreous hemorrhage occurring 38 years after cataract surgery. Case Rep Ophthalmol Med 2011;2011:340859.
2. Yamazoe K, Shimazaki-Den S, Otaka I, et al. Surgically induced necrotizing scleritis after primary pterygium surgery with conjunctival autograft. Clin Ophthalmol 2011;5:1609-11.
3. Pirouzian A. Management of pediatric corneal limbal dermoids. Clin Ophthalmol 2013;7:607-14.
4. Watts P, Michaeli-Cohen A, Abdolell M, et al. Outcome of lamellar keratoplasty for limbal dermoids in children. J AAPOS 2002;6:209-15.
5. Shen YD, Chen WL, Wang IJ, et al. Full-thickness central corneal grafts in lamellar keratoscleroplasty to treat limbal dermoids. Ophthalmology 2005;112:1955.
6. Cha DM, Shin KH, Kim KH, et al. Simple keratectomy and corneal tattooing for limbal dermoids: results of a 3-year study. Int J Ophthalmol 2013;6:463-6.
7. Yamazoe K, Shimazaki-Den S, Otaka I, et al. Surgically induced necrotizing scleritis after primary pterygium surgery with conjunctival autograft. Clin Ophthalmol 2011;5:1609-11
8. Yalçindag FN, Celik S, Ozdemir O. Repair of anterior staphyloma with dehydrated dura mater patch graft. Ophthalmic Surg Lasers Imaging 2008;39:346-7.
9. Ozcan AA, Bilgic E, Yagmur M, et al. Surgical management of scleral defects. Cornea 2005;24:308-11.
10. Polat N. Use of an Autologous Lamellar Scleral Graft to Repair a Scleral Melt After Mitomycin Application. Ophthalmol Ther 2014;3:73-6.
相关文章
Haisheng Zheng;Jingjing Huang,Overhanging glaucoma ff ltration bleb related to cataract surgeryYali Du;Lixia Sun;Mingzhi Zhang,The early change of corneal vertical coma and trefoil in 2.8-mm superior incision cataract surgeryHongpeng Li;Linxing Chen;Haili Fang;Hongxing Diao;Wenyan Liu,Analysis of different vision charts used for visual acuity assessment after retinal surgery