Age-determined referral criteria of myopia for large-scale vision screening
阅读量:1366
DOI:doi: 10.3978/ j.issn.1000-4432.2015.11.03
发布日期:2025-01-01
作者:
Hongjie Yu
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Age-determined referral criteria
myopia screening
receiver operating characteristic curve (ROC curve)
摘要
Background: This study aimed to explore the best screening measure of myopia and its associated optimal
referral criteria for children aged between 6 and 16.
Methods: After informed consent of cycloplegia was obtained, a total of 6,321 children aged between 6 and
16 from 53 primary or junior middle schools in Jiading District of Shanghai were included in our populationbased
study. Receiver operating characteristic (ROC) curve was performed to determine the best cutoff
points, sensitivities and specifi cities of diff erent screening tests, including uncorrected visual acuity (UCVA),
noncycloplegic autorefraction (NCAR) and the combination of these two tests.
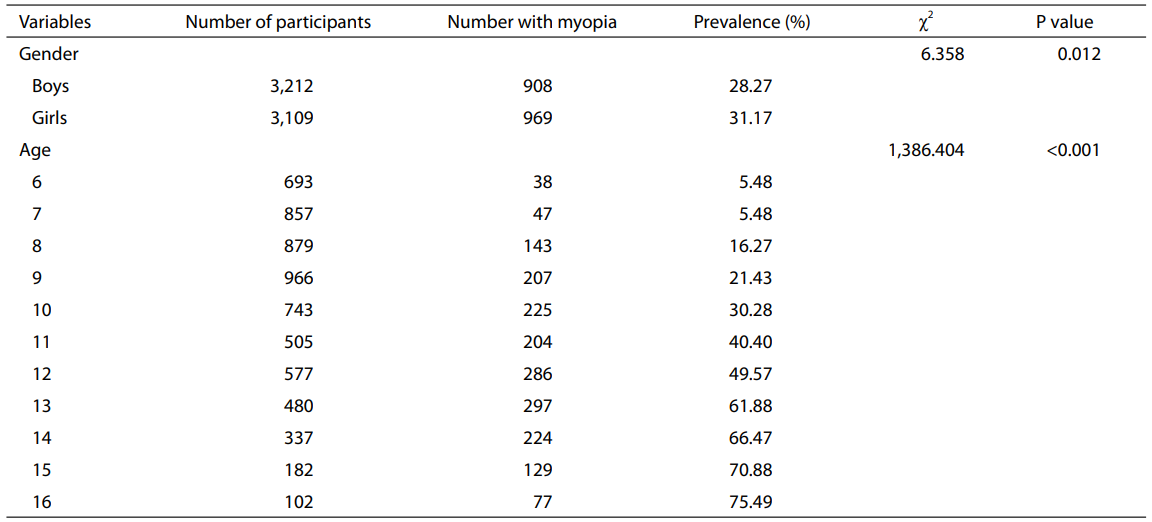
Results: There was significant difference in prevalence of myopia between boys and girls (χ2 =6.358, P=0.012). Compared with children of low age, the prevalence of older children was significantly higher
(χ2 =1,386.404, P<0.001). For the combination of UCVA and NCAR, the best cutoff point was UCVA
less than or equal to 0.2 logarithm of minimum angle of resolution (MAR) (20/30) and NCAR spherical
equivalent refraction (SER) less than or equal to ?0.75 diopters (D), with associated sensitivity and specifi city
of 75.0% and 85.0%, respectively, which were higher than those of UCVA and NCAR alone. After stratified
by age, the best cutoff points were varied among children. The accuracy for children aged between 9 and 12
was higher than that for other ages.
Conclusions: The best screening measure of myopia was the combination of UCVA and NCAR. The
optimal referral criteria of myopia for children should be age-determined.
全文
Introduction
Myopia, as the commonest refractive error, has become a
severe public health problem and shown a more and more
obvious low-age trend worldwide over the last decade(1-5). According to the latest report, the prevalence of
myopia in primary school children of Shanghai reached
42.6%, which was much higher than that of several years
ago(6-9). So it is important to detect myopic children
with feasible screening measure which has high sensitivity
and specificity to ensure early treatment. Some research
has reported the increased accuracy of the combination
of uncorrected visual acuity (UCVA) and noncycloplegic
autorefraction (NCAR) compared with either of the
two tests alone(10). In order to verify the accuracy
of this combination measure and further explore the
optimal referral criteria of myopia for different ages, the
vision screening data of all primary and junior middle school children who had signed the informed consent of
cycloplegia was collected and analyzed.
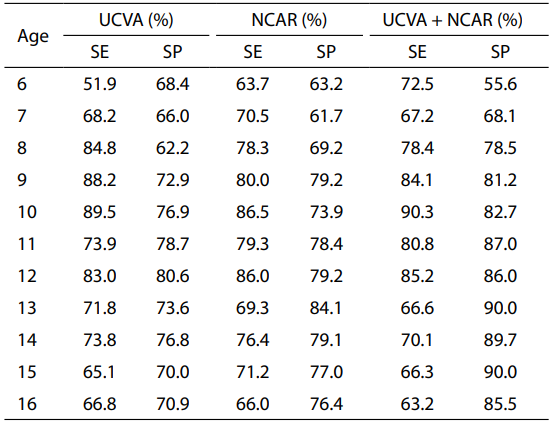
As shown in Table 2, after stratifi ed by age, the accuracy was different among ages. For all children aged between 7 and 16, the combination of UCVA and NCAR achieved higher SPs and similar SEs compared with these two tests alone. For children aged 6, the SP of the combination measure was 55.6%, which was lower than that of either of the two tests (68.4% and 63.2%, respectively), but the SE was much higher. Both SEs and SPs were over 80% for children aged between 9 and 12, which were relatively higher than those of other ages.
 UCVA, uncorrected visual acuity; NCAR, noncycloplegic
autorefraction; SE, sensitivity; SP, specifi city.
UCVA, uncorrected visual acuity; NCAR, noncycloplegic
autorefraction; SE, sensitivity; SP, specifi city.
 UCVA, uncorrected visual acuity; MAR, minimum angle
of resolution; NCAR, noncycloplegic autorefraction; D,
diopters.
UCVA, uncorrected visual acuity; MAR, minimum angle
of resolution; NCAR, noncycloplegic autorefraction; D,
diopters.
Subjects and methods
Subjects
A population-based cross-sectional study, which was approved by the Ethics Committee of Shanghai Eye Disease Prevention and Treatment Center, was conducted in Jiading District of Shanghai. A total of 53 primary and junior middle schools were included and all children were investigated. A total of 150 children were sampled randomly from each of the 53 schools from database. After those who refused cycloplegia were excluded, a total of 6,321 children aged between 6 and 16 were included.Methods
A total of 26 trained professional health workers from 13 Centers for Community Health Service undertook the vision screening. After visual acuity test, a Topcon KR8900 autorefractor (Topcon Company, Tokyo, Japan) was performed to achieve NCAR, which was followed by c ycloplegic refrac tion with 1% cyclopentolate hydrochloride. Children whose cycloplegic refraction spherical equivalent refraction (SER) was less than or equal to −0.50 diopters (D) were diagnosed as myopia.Statistical analysis
Epidata 3.1 statistical software was employed to input data and SPSS 17.0 was performed to draw receiver operating characteristic (ROC) curve for exploring the best cutoff points, sensitivities (SEs) and specificities (SPs) of different screening tests.Results
General information
Totally, 5,220 primary school children (aged between 6 and 12) and 1,101 junior middle school children (aged between 13 and 16) were recruited, including 3,212 boys and 3,109 girls, which accounted for 50.81% and 49.19% of all, respectively. After cycloplegic refraction, which was considered as golden standard for diagnosing myopia, 1,876 of 6,321 (29.68%) children were diagnosed as myopia. There was significant difference in prevalence of myopia between boys and girls (χ2 =6.358, P=0.012). Compared with children of low age, the prevalence of older children was significantly higher (χ2 =1,386.404, P<0.001). The detailed information of all children was presented in Table 1.
Table 1 General characteristics of the 6,321 participants
Comparison of accuracy of different screening tests
For all children, the general best cutoff point for UCVA was less than or equal to 0.2 logarithm of minimum angle of resolution (MAR) (20/30), with associated SE and SP of 77.4% and 74.3%, respectively. For NCAR, the general best cutoff point was SER less than or equal to −0.75 D, with associated SE and SP of 76.4% and 80.9%, respectively. After combining these two tests, the general best cutoff point was UCVA less than or equal to 0.2 logarithm of MAR and NCAR SER less than or equal to −0.75 D, with associated SE and SP of 75.0% and 85.0%, respectively.As shown in Table 2, after stratifi ed by age, the accuracy was different among ages. For all children aged between 7 and 16, the combination of UCVA and NCAR achieved higher SPs and similar SEs compared with these two tests alone. For children aged 6, the SP of the combination measure was 55.6%, which was lower than that of either of the two tests (68.4% and 63.2%, respectively), but the SE was much higher. Both SEs and SPs were over 80% for children aged between 9 and 12, which were relatively higher than those of other ages.
Table 2 Comparison of accuracy of diff erent screening tests for
children of all ages
Best cutoff points of combination measure for all ages
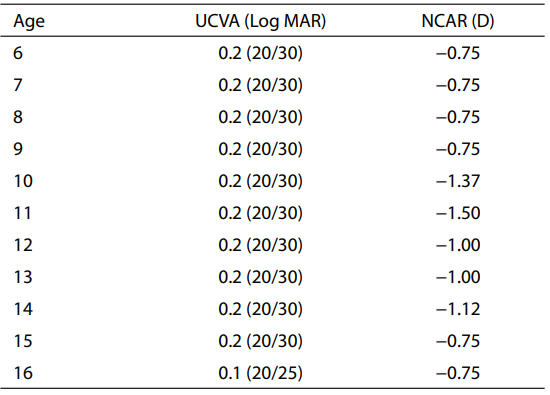
Table 3 offered the best cutoff points of the combination measure for all ages. For children aged from 6 to 9 and 15, the best cutoff point was UCVA less than or equal to 0.2 logarithm of MAR and NCAR SER less than or equal to −0.75 D, which was the same with the general best cutoff point. For children aged between 12 and 13, the best cutoff point was UCVA less than or equal to 0.2 logarithm of MAR and NCAR SER less than or equal to −1.00 D. The best cutoff points for other ages were different from each other. For children aged 10, 11 and 14, the best cutoff points were UCVA less than or equal to 0.2 logarithm of MAR and NCAR SER less than or equal to −1.37 D, −1.50 D and −1.12 D, respectively. For those aged 16, the best cutoff point was UCVA less than or equal to 0.1 logarithm of MAR (20/25) and NCAR SER less than or equal to −0.75 D.
Table 3 The best cutoff points of combination measure for
children of all ages
Discussion
More and more attention was paid to myopia of children
due to the high incidence and its increasing tendency(1,6-9,11,12). Some potential associations between myopia
and major age-related eye diseases were reported, such as
nuclear cataract, posterior subcapsular cataract and primary
open-angle glaucoma(13). So it is critical to detect children
with true myopia or with high risk of myopia in early age
accurately, which would lead to an early treatment and help
to relieve the long-term damage. However, the result of
UCVA was subject to be affected by environmental factors,
such as light intensity and reminding from people around
in reality, and often could not detect those with myopia
accurately, which means quite a few of missed diagnosis.
Cycloplegic refraction with retinoscopy and subjective refraction were usually used in most of professional
hospitals, but cycloplegic refraction with retinoscopy needs
high professional skills and rich experience, while subjective
refraction without cycloplegia is not accurate enough for
children, so both of these two methods are not suitable to
be used during large-scale screening. By contrast, NCAR
test is more objective, therefore, it is necessary to combine
NCAR test in order to increase the accuracy of myopia
screening(14-16). For controlling and even lowering the
incidence of myopia, a program on establishing individual
archives of ocular refractive development of children, which
was included in the agenda of local government to enhance
the public health system, was launched in Jiading District
in 2011 and completed at the end of 2013. According to
our study on this program, the SP of UCVA combined with
NCAR was 85.0%, which was much higher than that of the
two tests alone. Meanwhile, the SE of the combination kept
similar to that of UCVA and NCAR alone. In other words,
the combination measure achieved an increased accuracy,
which was in accordance with some researches before(10,17,18). Furthermore, our population-based study had a
larger sample size, which promised a reliable result.
In addition, the accuracy for children aged between 9 and 12 was relatively higher than that of other ages, indicating that the combination was more practical for children in this age group. The accuracy for those aged 6 and 7 was much lower than that for other ages, due to the stronger refraction adjustment ability and poor cooperation of younger children(19). Furthermore, we explored that the best cutoff points were age dependent for the measure of UCVA combined with NCAR. For children aged from 6 to 9 and 15, the best cutoff points were the same. Similarly, children aged 12 and 13 also shared the same best cutoff point. For other ages, the best cutoff points varied. With the progress of dynamic monitoring of children refractive development in the future, we would further examine the criteria and the associated accuracy for myopia screening. To find the risk factors of myopia and deliver targeted intervention after vision screening is important, some researches have reported the potential risk factors, such as lack of outdoor activities, heavy homework, wrong posture of reading and writing, long-time playing electronic products, and so on(8,9). In the following study, we would explore the myopia-related risk factors and feasible intervention based on the dynamic screening.
In conclusion, with an increased accuracy, the combination of UCVA and NCAR was more feasible to apply in large-scale myopia screening. The referral criteria of myopia for primary and junior middle school children should be age-determined.
In addition, the accuracy for children aged between 9 and 12 was relatively higher than that of other ages, indicating that the combination was more practical for children in this age group. The accuracy for those aged 6 and 7 was much lower than that for other ages, due to the stronger refraction adjustment ability and poor cooperation of younger children(19). Furthermore, we explored that the best cutoff points were age dependent for the measure of UCVA combined with NCAR. For children aged from 6 to 9 and 15, the best cutoff points were the same. Similarly, children aged 12 and 13 also shared the same best cutoff point. For other ages, the best cutoff points varied. With the progress of dynamic monitoring of children refractive development in the future, we would further examine the criteria and the associated accuracy for myopia screening. To find the risk factors of myopia and deliver targeted intervention after vision screening is important, some researches have reported the potential risk factors, such as lack of outdoor activities, heavy homework, wrong posture of reading and writing, long-time playing electronic products, and so on(8,9). In the following study, we would explore the myopia-related risk factors and feasible intervention based on the dynamic screening.
In conclusion, with an increased accuracy, the combination of UCVA and NCAR was more feasible to apply in large-scale myopia screening. The referral criteria of myopia for primary and junior middle school children should be age-determined.
基金
暂无基金信息
参考文献
1. Gursoy H, Basmak H, Yaz Y, et al. Vision screening in children entering school: Eskisehir, Turkey. Ophthalmic Epidemiol 2013;20:232-8.
2. Al Wadaani FA, Amin TT, Ali A, et al. Prevalence and pattern of refractive errors among primary school children in Al Hassa , Saudi Arabia. Glob J Health Sci 2012;5:125-34
3. Yingyong P. Risk factors for refractive errors in primary school children (6-12 years old) in Nakhon Pathom Province. J Med Assoc Thai 2010;93:1288-93.
4. Yared AW, Belaynew WT, Destaye S, et al. Prevalence of refractive errors among school children in gondar town, northwest ethiopia. Middle East Afr J Ophthalmol 2012;19:372-6.
5. Tu CY, Fu LJ, Fang YR, et al. A study on prevalence of myopia and its infl uencing factors among pupils. Zhejiang Journal of Preventive Medicine 2013;25:8-11.
6. Wang XW, Tan H, You XF, et al. Epidemiological characters of nearsightedness and vision care behaviors of primary school students in Shanghai. Maternal and Child Health Care of China 2013;24:3946-9.
7. Zhang KM. The myopia prevention of youth in Shanghai: current situation, problems and measures. Shanghai Journal of Preventive Medicine 2004;16:239-41.
8. Xu WY, Wang SM, Liu XR, et al. An evaluation of risk factors related to myopia among low-grade pupils in Shanghai. Chinese Journal of School Health 2008;29:681-5.
9. Xie HL, Xie ZK, Ye J, et al. Analysis of correlative factors and prevalence on China's youth myopia. Zhonghua Yi Xue Za Zhi 2010;90:439-42.
10. Ma Y, He X, Zou H, et al. Myopia screening: combining visual acuity and noncycloplegic autorefraction. Optom Vis Sci 2013;90:1479-85.
11. Ji CY. Status of impaired-vision and suspect-myopia in Chinese primary and secondary school students in 2005. Chinese Journal of School Health 2008;29:97-9.
12. Fan DS, Cheung EY, Lai RY, et al. Myopia progression among preschool Chinese children in Hong Kong. Ann Acad Med Singapore 2004;33:39-43.
13. Pan CW, Cheung CY, Aung T, et al. Diff erential associations of myopia with major age-related eye diseases: the Singapore Indian Eye Study. Ophthalmology 2013;120:284-91.
14. O'Donoghue L, Rudnicka AR, McClelland JF, et al. Visual acuity measures do not reliably detect childhood refractive error--an epidemiological study. PLoS One 2012;7:e34441.
15. Chu RY, Qu XM. Refraction is important procedure in the diagnose and treatment of eye diseases. Zhonghua Yan Ke Za Zhi 2010;46:961-3.
16. Choong YF, Chen AH, Goh PP. A comparison of autorefraction and subjective refraction with and without cycloplegia in primary school children. Am J Ophthalmol 2006;142:68-74.
17. Lai YH, Tseng HY, Hsu HT, et al. Uncorrected visual acuity and noncycloplegic autorefraction predict signifi cant refractive errors in Taiwanese preschool children.
Ophthalmology 2013;120:271-6.
18. He XG, Zhu JF, Lu LN. Combined Use of Uncorrected Visual Acuity and Noncycloplegic Autorefraction for Myopia Screening in Children. Chinese Journal of School Health 2010;31:960-2.
19. Qu XH, Zhong DD, Liu WM, et al. The comparison of refraction with and without cycloplegic in preschool children. Guide of China Medicine 2011;9:85-6.
相关文章
Shuiming Yu;Hongxing Diao;Junwen Zeng,Analysis of the Prevalence and Situation of Myopia in Adolescents from South China赵兰琴;肖薇;王铭薇;杨雅涵;林铎儒;庞健宇;丘蔚晴;吴悦;何雨春;胡建民;林浩添,Lifestyle and myopia among primary school students in urban areas of Fujian following implementation plan for comprehensive prevention and control of myopia of children and dolescents: a cross-sectional studyVictoria M. Sánchez;Rafael Iribarren;Santiago G. Latino;Victor E. Torres;Ana L. Gramajo;María N. Artal;María B. Yadarola;Patricia R. Garay;José D. Luna;Claudio P. Juarez,Prevalence of refractive errors in Villa Maria, Córdoba, Argentina