Hydrostatic pressure changes during simulated lacrimal sac massage on a congenital nasolacrimal duct obstruction (CNLDO) model
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
摘要
Objective: Congenital nasolacrimal duct obstruction (CNLDO) affects 5%-20% of infants. Lacrimal sac massage is considered the first-line therapy for CNLDO, yet there is a lack of quantitative comparisons among different massage techniques. The aim of this study is to quantitatively evaluate the changes in hydrostatic pressure at the inferior nasolacrimal duct (NLD) orifice during the application of different lacrimal sac massage techniques for CNLDO, using a validated simulation model. Methods: This was an experimental biomechanical study that used a CNLDO model equipped with sensors. The simulation was conducted in a laboratory setting at an academic ophthalmology center. First, seven expert ophthalmologists validated the model, and then three of them performed the massage techniques. A total of four massage techniques were applied: Technique I (Horizontal), Technique II (Vertical), Technique III (45° Oblique), Technique IV (Crigler’s, inferomedial). The primary outcome measure was the hydrostatic pressure (mmHg) at the lower NLD orifice during the application of each massage technique. Secondary measures included force vectors and the degree of compression of the common canaliculus. Results: The Crigler’s technique (IV) generated the highest median and maximum hydrostatic pressure at the lower NLD orifice, followed by Technique III (45° oblique). In contrast, Techniques I and II produced significantly lower pressures. Sensor data collected during the application of maximal Crigler’s pressure (0.7 N at NLD orifice) showed several key findings. There was a concurrent force >0.3 N over the common canaliculus, which effectively prevented reflux. Additionally, there was a rapid application of a 1.9 N force over the lacrimal sac directed inferomedially, resulting in a 0.2 N pressure at the sac/NLD junction. During the generation of maximal Crigler’s pressure: 1) A force of 0.7 N was recorded at NLD orifice; 2) There was a concurrent 1.9 N inferomedial force applied to the lacrimal sac. 3) A pressure of 0.2 N was measured at the sac/NLD junction. In all applications of Crigler’s technique, the compression of the common canaliculus remained >0.3 N, which is the threshold for preventing reflux. Conclusions: This quantitative study demonstrates that Crigler’s lacrimal sac massage generates significantly higher hydrostatic pressure at the lower NLD orifice compared to alternative techniques, while simultaneously maintaining a compression of the common canaliculus that prevents reflux. These findings provide biomechanical evidence to support the use of Crigler’s technique as the optimal massage method for the treatment of CNLDO. Clinical adoption of this technique may lead to improve rates of obstruction clearance and a reduced need for invasive procedures.
全文
HIGHLIGHTS
1. Achieved direct and quantitative measurement of pressure changes at the lower opening of the nasolacrimal duct (NLD)
• This study successfully developed and validated a highly realistic simulation model of the lacrimal duct’s anatomy and fluid dynamics. It overcame, the technical barriers to in-vivo measurement, precisely quantifying the hydrostatic pressure changes induced by different massage techniques at the lower opening of the NLD. This fills a long-standing gap in the field by providing direct and quantitative data.
2. Constructed a multifunctional innovation platform integrating research and training
• The invented model serves not only as a research tool but also as an efficient standardized teaching and training system. It can be objectively and reproducibly used to train young physicians and the families of pediatric patients, ensuring the accuracy and consistency of massage techniques. This fundamentally addresses the issue of uncertain therapeutic outcomes caused by variations in the operator’s techniques.
3. Provided an evidence-based decision-making basis for clinical practice
• Through systematic model experiments, this study scientifically compared the pressure effects of different massage techniques and the Crigler technique. The research findings directly translate abstract techniques into concrete pressure data, offering clinicians objective and quantitative scientific evidence for selecting the most optimized and effective massage protocols. This promotes a shift in treatment from “experience-dependent” to “evidence-driven”.
4. Pioneered a standardized and refined research methodology for lacrimal sac massage techniques
• This study established a comprehensive “simulation-measurement-validation-assessment” methodological framework. This framework lays a solid foundation for future in-depth exploration of the quantitative relationships between massage parameters (such as force, direction, and frequency) and therapeutic outcomes, as well as the development of novel optimized techniques. It opens up a new direction for quantitative research in this field.
Congenital nasolacrimal duct obstruction (CNLDO) is a common pediatric ophthalmic disorder. It is characterized by the failure of tears to drain into the nasal cavity because the nasolacrimal duct (NLD) is not patent at birth, which subsequently leads to epiphora (excessive tearing). Reported incidence rates of CNLDO in infants under one year of age range from 5% to 20%,[1] with an average incidence rate of approximately 6%.[2] This condition makes infants more susceptible to infections, which can result in either chronic or acute dacryocystitis.[3] Furthermore, in severe cases, the infection can spread to the orbital tissues or even intracranially, causing significant complications. These complications can have a profound impact on the physical and psychological well-being of affected children. Lacrimal sac massage serves as the initial conservative treatment option for CNLDO, and there is evidence to support its effectiveness.[4] Several distinct massage techniques have been described in the literature. In 1923, Crigler’s lacrimal sac massage technique was first reported in JAMA (Journal of the American Medical Association), and it achieved favorable results.[5] However, more than a century has passed since then, and there are no quantitative studies reported on the hydrostatic pressure changes generated at the inferior opening of the nasolacrimal duct by these various massage techniques. Such quantitative data is of vital importance as it can provide crucial guidance for clinicians in selecting the most appropriate massage method. This study aimed to develop and validate a simulation model specifically designed for lacrimal sac massage in the context of CNLDO. The primary objective was to quantify hydrostatic pressure changes at the lower NLD orifice that are induced by different massage techniques applied to the model.
Methods
Design and fabrication of the simulation model
The CNLDO simulation model system comprised several key components: a 3-month-old infant skull model, uncured liquid silicone (0° silicone), a silicone nasolacrimal duct model, and a pressure sensing system. The pressure sensing system included pressure sensors, a digital display, and a power supply. It was capable of measuring forces in the range of 0-100.0 N with a resolution of 0.1 N, along with other necessary equipment.
To establish a CNLDO model, we selected standard cranial computed tomography (CT) scans without contrast. These scans were obtained from a healthy, full-term, 3-month-old infant who had normal osseous development and no observed bony deformities or variations. The study was approved by the Ethical Review Board of the Third Medical Center, Chinese PLA General Hospital (KY2023~012). It adhered to the principles of the Declaration of Helsinki. The subject voluntarily participated in this study and provided informed consent by infants’ guardians.
Based on these CT scans, a 3D digital model was constructed. The right eyeball and the surrounding periocular soft tissues were digitally removed to clearly expose the right lacrimal sac fossa and the bony nasolacrimal canal. Subsequently, a physical infant skull model was fabricated using 3D printing technology with resin material. This model was then split along the midsagittal plane.
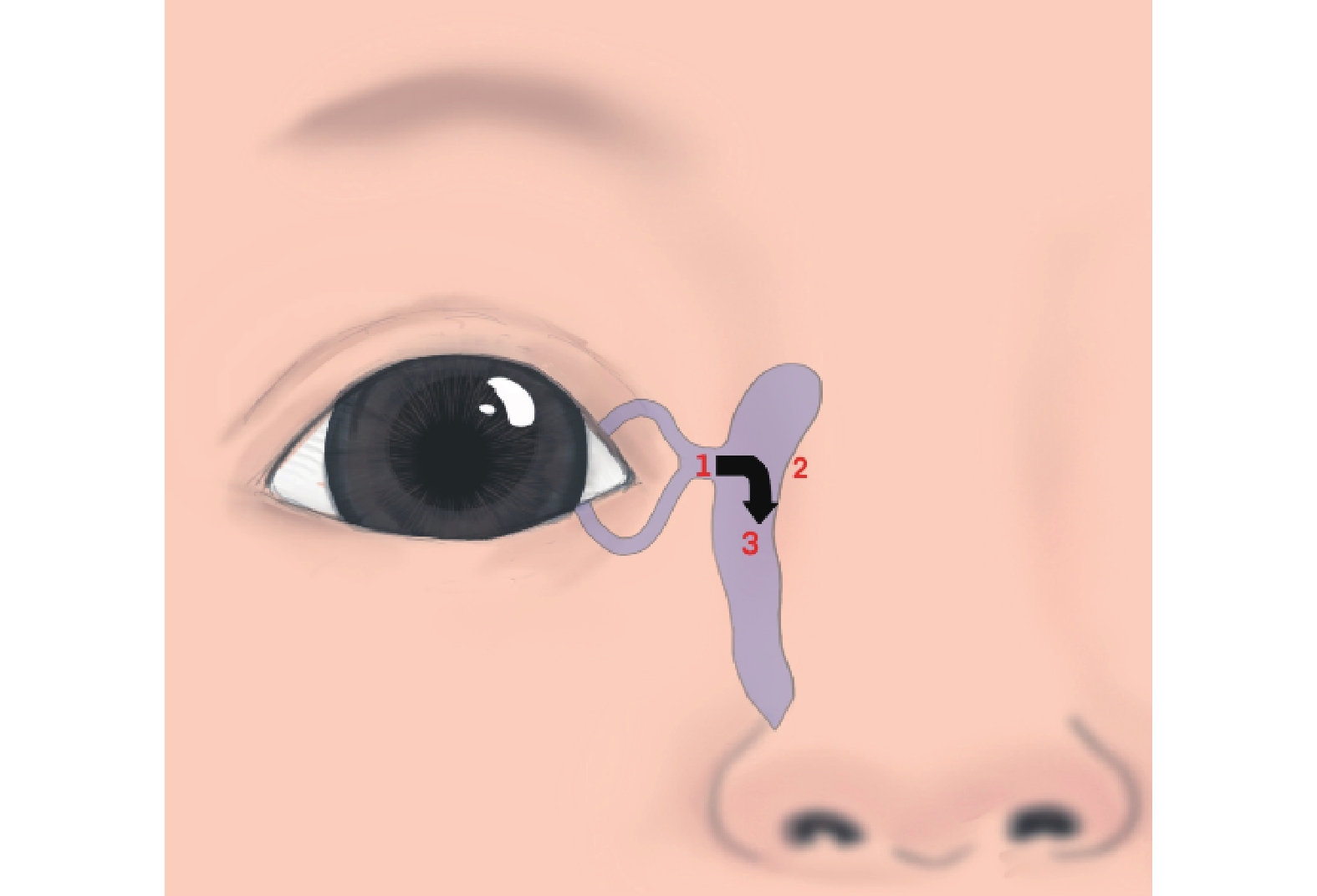
Three pressure sensor probes were strategically positioned at important anatomical sites: posterior to the common canaliculus, superonasal to the lacrimal sac (within the lacrimal sac fossa), and at the junction of the lacrimal sac and the nasolacrimal duct. A transparent silicone elastomer, whose refractive index matched that of the surrounding model material, was then used to cast the nasolacrimal duct model, with the sensor probes embedded within it (Figure 1).

The silicone nasolacrimal duct model was precisely placed within the bony nasolacrimal canal of the skull model. This arrangement guaranteed accurate contact between crucial anatomical points on the duct model-specifically, the area posterior to the common canaliculus, the nasal side of the lacrimal sac, and the junction of the lacrimal sac and the nasolacrimal duct and their corresponding pressure sensor probe, which were embedded within the skull structure.
To simulate CNLDO, an additional pressure sensor probe was placed inside the lumen at the inferior opening of the nasolacrimal duct. After that, the entire duct system was filled with physiological saline that had been stained blue (to approximate the density of tear fluid) by injecting it into the canaliculus.
Subsequently, uncured liquid silicone (0° silicone) was poured into the orbital cavity to encase the duct model and sensors. The silicone was filled to a level that ended 5 mm anterior to the silicone tubing representing the common canaliculus. The surface of the cured silicone was carefully contoured to replicate the anatomical appearance of the contralateral orbit, based on the original 3D model (Figure 2).
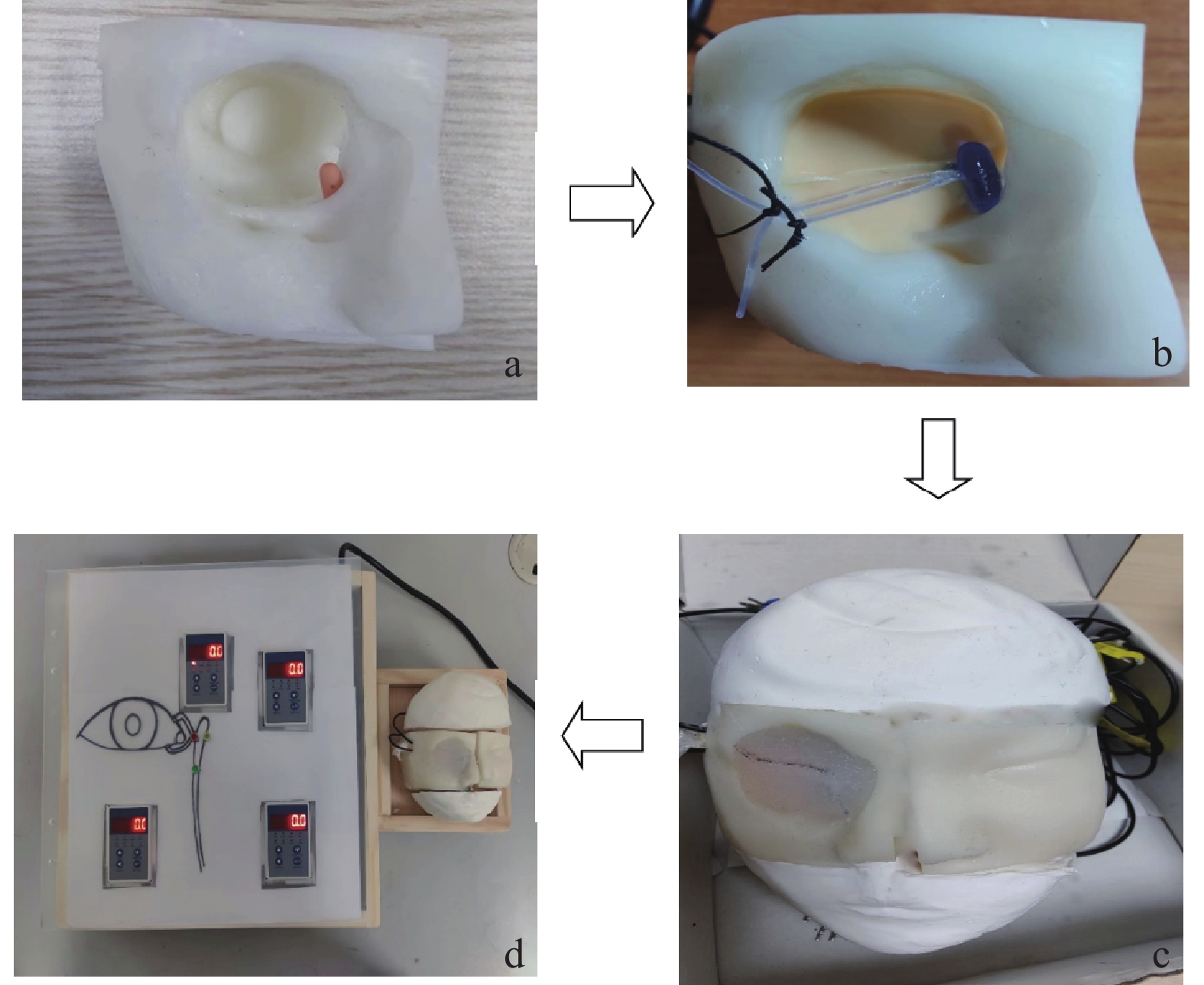
After the model was fully completed, seven ophthalmologists with extensive experience in pediatric lacrimal disorders were invited to evaluate the simulation. These experts assessed multiple aspects of the model, including its anatomical shape and size, the degree of tactile realism if offered, the sensor sensitivity to massage maneuvers, and sensor stability. All evaluations were conducted using a standardized 5-point Likert scale (Table 1).
|
Please evaluate your experience using the following scale: |
|
1 =strongly disagree, 2 = disagree, 3= neutral, 4 =agree, 5= strongly agree |
|
1. The overall size of the model was appropriate for the lacrimal sac techniques. |
|
2. An adequate number of landmark structures were present. |
|
3. The location and feel of the landmark structures were suitably realistic. |
|
4. The materials looked and felt appropriately realistic. |
|
5. The model was easy to use. |
|
6. The model was suitable to teach the preparation and steps required to perform the lacrimal sac techniques. |
|
7. The model was suitable to give young ophthalmologists and parents a general idea of the actual tactile experience when performing these lacrimal sac techniques. |
|
8. I feel that this model would be helpful for young ophthalmologists and parents to practice these skills before performing them on children. |
|
9. I feel that this model is adequate to assess young ophthalmologists and parents performance of the lacrimal sac techniques stated. |
|
10. I have concerns that this model could teach young ophthalmologists and parents poor technique. |
|
Comments (please explain negative or neutral ratings so that the model can be improved): |
Massage technique design and experimental protocol
Given that Crigler’s lacrimal sac technique has demonstrated favorable outcomes in prior research, four different lacrimal sac massage techniques were devised based on this approach:
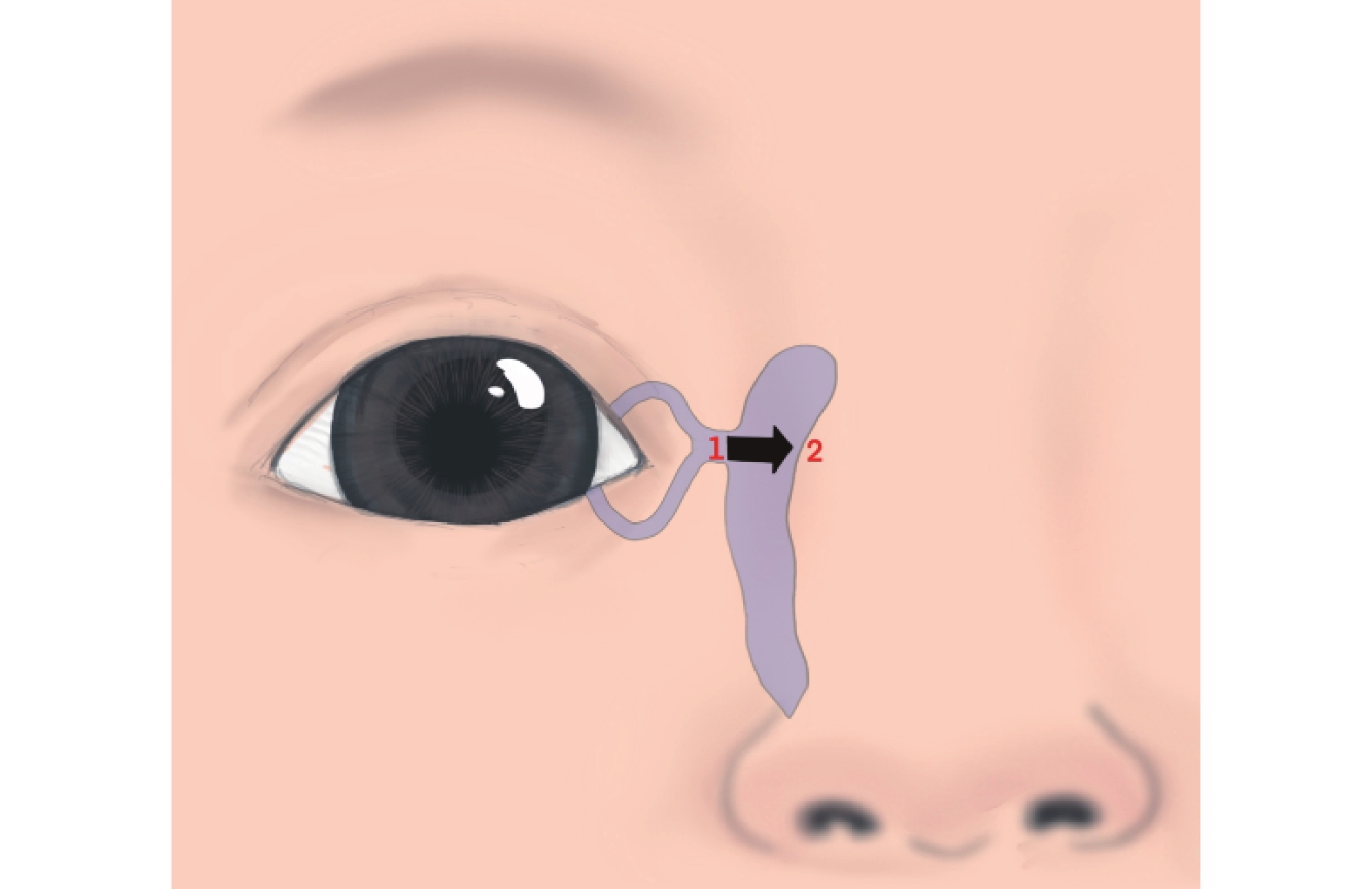
•Technique I (Horizontal Massage): The thumb pad exerted a force >0.3 N over the common canaliculus. Subsequently, horizontal pressure was applied in a nasal direction over the lacrimal sac. Pressure readings were recorded from the sensor located at the lower NLD orifice (Figure 3).
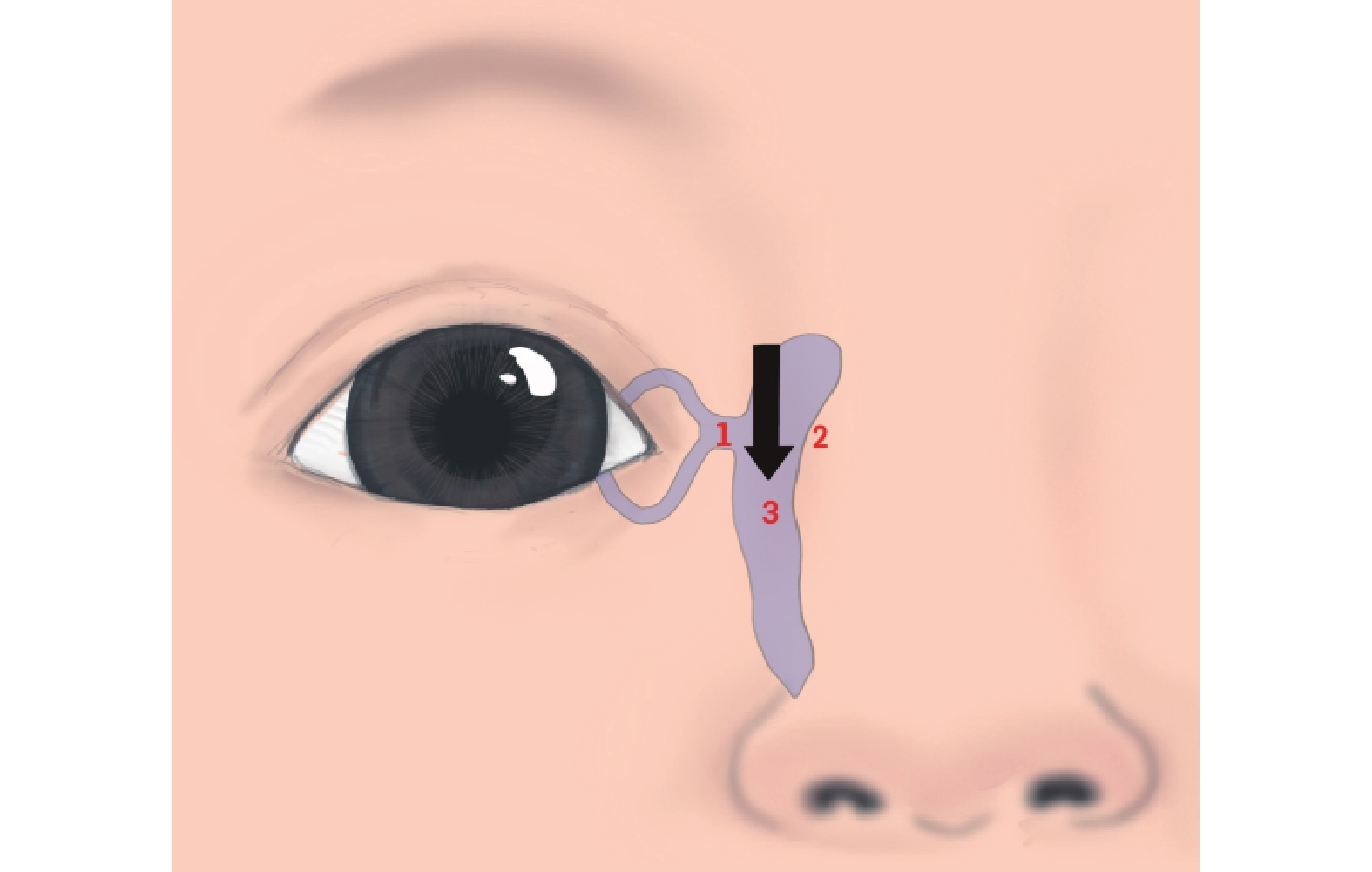
•Technique II (Vertical Massage): The thumb pad applied direct downward pressure over the lacrimal sac, aiming towards the NLD. Pressure readings were taken from the sensor at the lower NLD orifice (Figure 4).
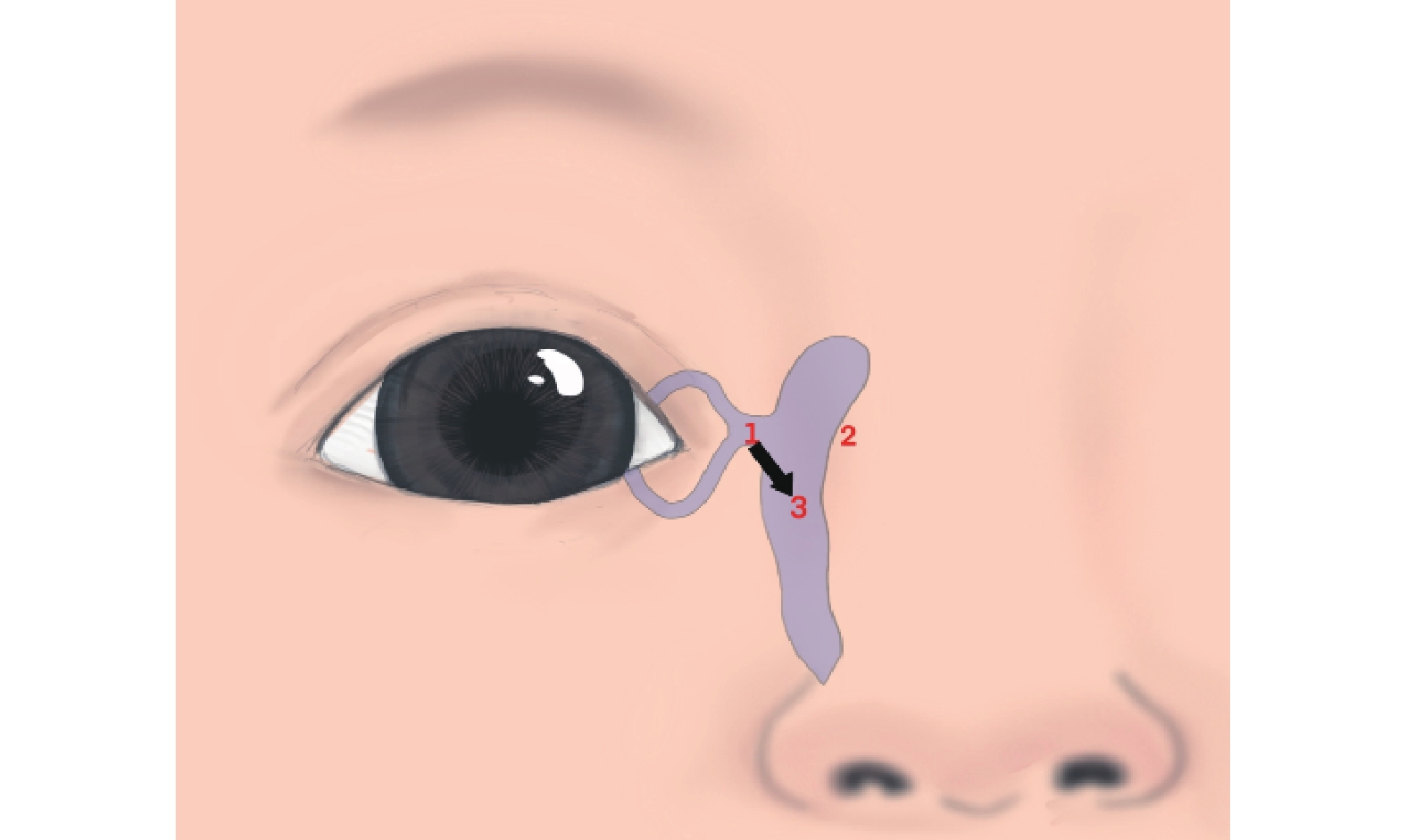
•Technique III (45° Oblique Massage): The thumb pad applied a force >0.3 N over the common canaliculus. Then, oblique pressure was applied in an inferomedial direction at a 45° angle (towards the nasal tip). Pressure readings were recorded from the sensor at the lower NLD orifice (Figure 5).
•Technique IV (Crigler’s Technique): The thumb applied a force >0.3 N over the common canaliculus. This was followed sequentially by horizontal pressure in a nasal direction over the lacrimal sac and then anteromedial pressure towards the NLD. Pressure readings were recorded from the the sensor at the lower NLD orifice (Figure 6).
Three ophthalmologists performed all the maneuvers using their right thumb. Each technique was applied in three consecutive repetitions per set. For each repetition within a set, the highest hydrostatic pressure (the maximum instantaneous value) generated at the lower NLD orifice was recorded. This procedure was repeated for ten independent sets per technique, resulting in the dataset presented in this study. This experimental approach was specifically designed to simulate the biomechanical action. In this action, the fluid pressure within the lacrimal sac has the potential to dislodge the obstruction at the lower NLD orifice, thereby achieving the therapeutic goal in cases of congenital nasolacrimal duct obstruction.
Statistical analysis
The survey data were analyzed using descriptive statistics, encompassing both median and mean values. The highest hydrostatic pressure values generated by the four massage techniques were assessed for normality using the Shapiro-Wilk test. Upon conducting the test, it was determined that the data exhibited a non-normally distributed (P<0.05). Consequently, inter-group comparisons were performed using the non-parametric Kruskal-Wallis test. Statistical significance was defined as P<0.05. All the statistical analyses were performed using IBM SPSS Statistics software (version 23).
Results
Model evaluation
The assessment results regarding the model’s dimensional accuracy, tactile fidelity, as well as sensor sensitivity and stability during massage, as evaluated by the expert panel, presented in Table 2. These results clearly demonstrate the simulation system’s favorable overall performance.
|
Survey Statement |
Strongly Disagree n (%) |
Disagree n (%) |
Neutral n (%) |
Agree n (%) |
Strongly agree n (%) |
|
1. The overall size of the model was appropriate for the lacrimal sac techniques. |
|
|
|
1(14) |
6(86) |
|
2. An adequate number of landmark structures were present. |
|
|
|
2(29) |
5(71) |
|
3. The location and feel of the landmark structures were suitably realistic. |
|
|
|
3(43) |
5(71) |
|
4. The materials looked and felt appropriately realistic. |
|
|
2(29) |
3(43) |
3(43) |
|
5. The model was easy to use. |
|
|
|
2(29) |
5(71) |
|
6. The model was suitable to teach the preparation and steps required to perform the lacrimal sac techniques. |
|
|
|
3(43) |
4(57) |
|
7. The model was suitable to give young ophthalmologists and parents a general idea of the actual tactile experience when performing these lacrimal sac techniques. |
|
|
1(14) |
2(29) |
4(57) |
|
8. I feel that this model would be helpful for young ophthalmologists and parents to practice these skills before performing them on children. |
|
|
|
3(43) |
4(57) |
|
9. I feel that this model is adequate to assess young ophthalmologists and parents performance of the lacrimal sac techniques stated. |
|
1(14) |
1(14) |
1(14) |
4(57) |
|
10. I have concerns that this model could teach young ophthalmologists and parents poor technique. |
2(29) |
2(29) |
3(43) |
|
|
Data analysis
Based on preliminary experimental findings, we established a minimum threshold pressure of 0.3 N to be applied over the common canaliculus. This was done to prevent retrograde fluid flow into the canaliculi. Utilizing the validated simulation model, each of the four massage techniques was applied with three consecutive compressions per set. For each compression within a set, we recorded the highest hydrostatic pressure, which refers to the maximum instantaneous value, generated at the lower NLD orifice. This procedure was repeated for ten independent sets of each technique. Subsequently, for comparative analysis, we calculated the median and maximum values of the recorded highest pressures across all sets for each technique (Table 3).
|
F/N |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
|
Technique I |
0.1 |
0.0 |
0.1 |
0.0 |
0.1 |
0.0 |
0.0 |
0.0 |
0.0 |
0.1 |
|
Technique II |
0.2 |
0.1 |
0.2 |
0.3 |
0.2 |
0.1 |
0.1 |
0.1 |
0.2 |
0.1 |
|
Technique III |
0.5 |
0.6 |
0.6 |
0.5 |
0.5 |
0.6 |
0.6 |
0.5 |
0.5 |
0.5 |
|
Technique IV |
0.6 |
0.7 |
0.7 |
0.7 |
0.6 |
0.6 |
0.6 |
0.7 |
0.7 |
0.7 |
Inter-group comparisons were conducted using the Kruskal-Wallis test, which is a non-parametric analysis of variance for multiple independent samples. Statistical significance was set at P<0.05, and the relevant results are presented in Table 4.
|
Group |
Median(P25, P75) |
the Kruskal-Wallis test |
|
|
Mean |
P |
||
|
TechniqueⅠ |
0.00(0.00,0.10) |
6.50 |
<0.001 |
|
TechniqueⅡ |
0.15(0.10,0.20) |
14.50 |
|
|
TechniqueⅢ |
0.55(0.50,0.60) |
26.50 |
|
|
TechniqueⅣ |
0.70(0.60,0.70) |
34.50 |
|
The median (interquartile range, IQR) values of hydrostatic pressure at the inferior opening of the nasolacrimal duct, induced by the four techniques were as follows: For Technique I, it was 0 (0, 0.10); for Technique II, 0.15 (0.10, 0.20); for Technique III, 0.55 (0.50, 0.60); and for Technique IV, 0.70 (0.60, 0.70). The Kruskal-Wallis test revealed statistically significant differences in the overall pressure distributions among the four groups (P<0.001). Specifically, Crigler’s lacrimal sac technique (Technique IV) generated the highest instantaneous hydrostatic pressure at the inferior opening of the nasolacrimal duct. The oblique 45° pressure technique (Technique III) produced the second highest pressure value. In contrast, both the simple horizontal pressure technique (Technique I) and the simple vertical pressure technique (Technique II) resulted in significantly lower instantaneous hydrostatic pressures at the inferior opening of the nasolacrimal duct.
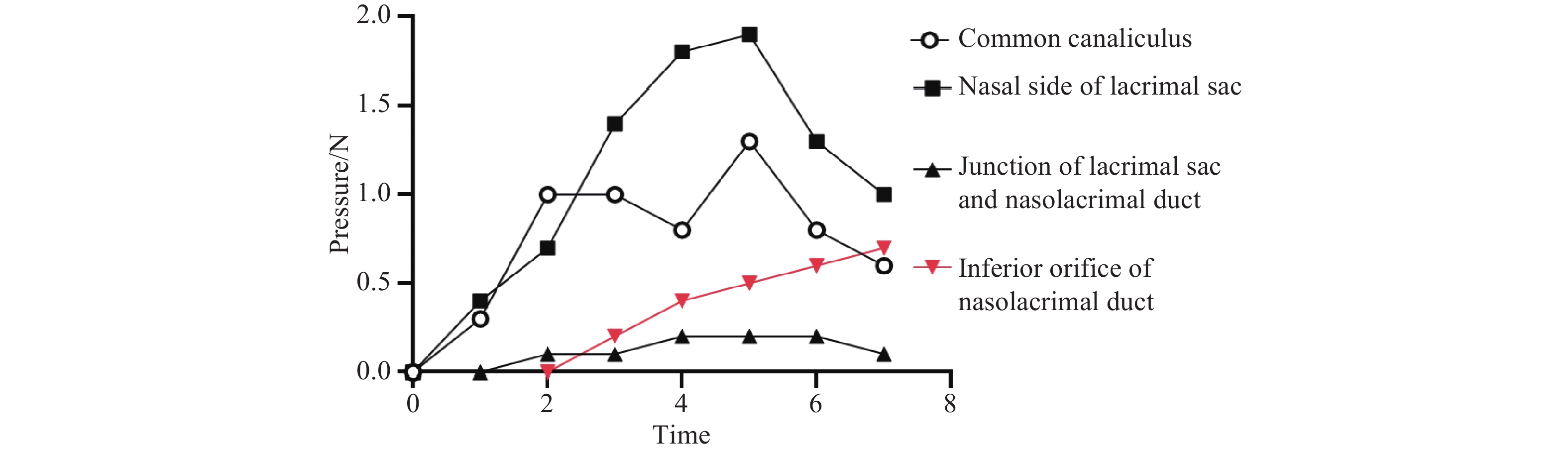
An analysis of data from the three additional pressure sensors showed that the maximum instantaneous hydrostatic pressure recorded at the inferior opening of the nasolacrimal duct (0.7 N) occurred under specific force conditions. This peak pressure was attained when the force applied at the common canaliculus exceeded 0.3 N, while simultaneously, a rapid force application to the lacrimal sac reached 1.9 N, followed immediately by a swift downward pressure towards the nasolacrimal duct. Crucially, the highest pressure (0.7 N) at the inferior opening coincided with the pressure measured within the lacrimal sac/nasolacrimal duct region registering 0.2 N. This pressure profile is illustrated in Figure 7.
Discussion
CNLDO primarily arises from a mechanical blockage caused by a delayed opening of the valve of Hasner, a membranous structure situated at the distal inferior opening of the NLD where it enters the inferior meatus.[2] In cases of CNLDO, the obstruction of this pathway hinders tear outflow, leading to tear accumulation on the ocular surface and the characteristic symptom of epiphora.[6-7] This condition not only has a detrimental impact on normal visual development but also predisposes infants to infection, potentially resulting in chronic or acute dacryocystitis.[3] The management of CNLDO encompasses a variety of strategies, which can be broadly classified into non-surgical and surgical interventions. Non-surgical options include lacrimal sac massage, topical ocular medications, and lacrimal irrigation. Surgical management generally favors minimally invasive procedures such as probing, laser-assisted dacryoplasty, endoscopic valve of Hasner incision, and endoscopic dacryocystorhinostomy.[4] Despite this range of therapeutic approaches, standardized selection criteria for CNLDO treatment remain a subject of controversy. Treatment decisions require a multifactorial assessment, considering factors such as the infant’s age, the severity of symptoms, and associated complications, as well as parental compliance and acceptance of surgical risks. The therapeutic principle involves increasing the hydrostatic pressure within the lacrimal drainage system to overcome the membranous obstruction at the distal NLD.[8] Clinical evidence demonstrates that occluding the common canaliculus prevents reflux into the canaliculi, allowing for the maximal application of force to the lacrimal sac. This maneuver generates elevated pressure within the sac, directing fluid flow towards the NLD. This pressurized flow may facilitate the rupture of the obstructing membrane at the NLD orifice, thereby achieving the therapeutic goal of treating CNLDO.[9]
Simulation experiments using our CNLDO model demonstrated that Crigler’s lacrimal sac technique generates significantly higher pressure at the inferior NLD opening compared to other techniques, suggesting greater therapeutic potential for CNLDO.[10-11] Crucially, the highest instantaneous hydrostatic pressure at the inferior opening was achieved under specific force dynamics. By occluding the common canaliculus to prevent reflux into the canaliculi, a rapid medial (nasal) pressure applied to the lacrimal sac reached 1.9 N. At the same time, a swift direction, applying downward pressure towards the NLD, resulted in a pressure of 0.2 N at the junction of the lacrimal sac and NLD. This specific combination of forces generated the maximum recorded instantaneous hydrostatic pressure at the target area.
This study aims to investigate the influence of various massage techniques on the hydrostatic pressure at the distal orifice of the NLD by monitoring this parameter during lacrimal sac massage. Since the lacrimal sac is located within the bony lacrimal fossa, repeated simulated massage trials on a model demonstrated that compressing the common canaliculus with a force greater than 0.3 N occludes its lumen. Under this condition, finger pressure applied to the lacrimal sac prevents fluid reflux into the canaliculi and directs most of the fluid into the NLD. When the lacrimal sac is compressed against the medial bony wall, minimizing its volume, further increases in pressure over the sac do not significantly change the hydrostatic pressure at the distal NLD orifice. Therefore, monitoring the hydrostatic pressure at this site ensures consistency when comparing different massage techniques.
A compressive force exceeding 0.3 N at the common canaliculus is necessary to generate hydrostatic pressure at the distal NLD orifice that is therapeutically effective. This finding explains why, in clinical practice, some infants do not respond to massage therapy even when the technique and direction of compression are correct—insufficient force may compromise treatment outcomes. To address this issue, the model incorporates a training function that guides caregivers to apply the appropriate force range during practice. Regarding calibration, the experimental setup requires this procedure, which is facilitated by our model through a zero-reset functionality for all measurement points prior to operation.
Furthermore, we observed minimal temporal variation in the pressure profile at the junction of the lacrimal sac and the NLD, with highest pressure values consistently remaining below 0.2 N. This pressure limitation may be due to the near-parallel orientation of fluid flow vectors relative to the duct wall in this region.
While the CNLDO simulation model cannot fully replicate the complexity of human tissue—using 3D-printed resin for craniofacial bones and soft tissues and 0-degree silicone to simulate medial orbital structures—these materials exhibit high biomimetic fidelity to human anatomy. Future advancements may focus on improving the model’s fidelity through optimized silicone polymers, multilayer composites, or reusable synthetic tissues to more accurately replicate human lacrimal duct tissue.[12] A 3-month-old infant(full-term, vaginal delivery) was selected as representative mainly because this age group shows the highest clinical presentation rate and treatment success rate for CNLDO.[9] CT scans confirmed the absence of lacrimal system anomalies in this infant, with bony nasolacrimal canal dimensions (length and width) in line with established literature values.[4] Following a consensus review by an expert panel, this case was deemed representative based on prior research and clinical evidence.
The CNLDO simulation model developed from the CT data and anatomy of a single infant represents a preliminary investigation. To account for uniqueness and individual variability, future clinical practice could incorporate CT imaging for each infant requiring lacrimal sac massage. This would enable the creation of personalized 3D-printed models, providing clinicians with a detailed anatomical understanding. Such individualized models would facilitate more precise massage techniques for infants with anatomical anomalies or variations. Crucially, infants with bony CNLDO must be excluded, as lacrimal sac massage is ineffective for this subtype.[8,13] Moreover, personalized models could empower caregivers to correct improper massage techniques (e.g., force, angle, location) through guided practice, even without direct professional supervision, potentially improving success rates. By rigorously accounting for individual anatomical differences, this approach could significantly reduce clinical decision-making errors arising from overlooked variability. Critically, infants with anomalies or variations may achieve effective treatment through customized technique adjustments, highlighting the substantial clinical relevance of personalized simulation modeling.
During the model calibration phase, the device was calibrated by seven senior physicians with extensive experience in diagnosing and treating pediatric lacrimal duct disorders. These experts formed a panel to comprehensively evaluate the model’s realism and functional completeness, ensuring its reliability and simulation accuracy. Although the surface area of an adult thumb is generally sufficient to cover the medial canthus of a child, operators were instructed to apply pressure specifically using the central region of the thumb pad—the primary and highest load-bearing area, which has a relatively limited contact zone. Pressure was applied along predefined paths and trajectories tailored to each massage technique to minimize subjective variability and improve precision. Additionally, repeated trials performed by each operator helped mitigate the impact of random variations on experimental outcomes. In the experimental phase, three ophthalmologists, trained uniformly, performed four massage techniques on the pre-validated model. This approach helped minimize operators variability and enhanced the consistency of experimental results.
The design and fabrication of this CNLDO simulation model provides exceptional three-dimensional visualization and significant didactic utility. It offers an intuitive perspective on the spatial relationships between the NLD and adjacent nasal structures. Furthermore, the model serves as a valuable adjunct to traditional anatomical atlases, facilitating enhanced comprehension and learning. This tangible representation significantly improves students’ spatial understanding of complex anatomy, demonstrating clear superiority for clinical education over purely two-dimensional resources. Consequently, the model has broad applicability in clinical training settings, particularly for visualizing intricate anatomical relationships.
Based on the findings, the following conclusions can be drawn: 1) A simulation model for lacrimal sac massage in CNLDO was successfully designed and fabricated. This model enables quantitative analysis of massage techniques and serves as an effective tool for teaching and training modules in CNLDO management. 2) Within the simulated CNLDO environment, multiple massage techniques were biomechanically evaluated. Data analysis confirmed that Crigler’s lacrimal sac technique generates the highest instantaneous hydrostatic pressure at the inferior NLD opening, providing a quantitative basis for evidence-based technique selection in clinical practice.
Correction notice
None
Acknowledgements
None
Author contributions
(I) Conception and design: Hai Tao, Ji Hao
(II) Administrative support: Hai Tao
(III) Provision of study materials or patients: Hai Tao, Ji Hao
(IV) Collection and assembly of data: Ji Hao
(V) Data analysis and interpretation: Hai Tao
(VI) Manuscript writing: All authors
(VII) Final approval of manuscript: All authors
Conflict of interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form.
Patient consent for publication
None
Ethical statement
The study was approved by the Ethical Review Board of the Third Medical Center, Chinese PLA General Hospital (KY2023-012).
Provenance and peer review
This article was a standard submission to our journal. The article has undergone peer review with our anonymous review system.
Data sharing statement
None
Open access statement
This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License(CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited(including links to both the formal publication through the relevant DOI and the license).