Conjunctivo-canaliculo-cysto-rhinostomy: repurposing an orbital mucocele as a neo-lacrimal conduit in congenital lacrimal agenesis
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
摘要
Background: Congenital absence of the lacrimal sac and nasolacrimal duct (congenital lacrimal drainage agenesis) brings special diagnostic and surgical challenges, especially when patients have persistent epiphora and cystic change in the inferomedial orbit. Since conventional dacryocystorhinostomy (DCR) needs a definable lacrimal sac to make a new drainage ostium into the nasal cavity, standard DCR may not be possible when there is true lacrimal sac/nasolacrimal duct agenesis. In this case, we need a reconstructive strategy that can restore tear outflow and also respect the patient’s congenital anatomy. We report a reconstructive approach-conjunctivo-canaliculo-cysto-rhinostomy (CCCR). When the native lacrimal sac is absent, it reuses an existing inferomedial orbital cystic cavity as a new lacrimal conduit to re-establish drainage. Methods: This study is a case report of a single patient from a tertiary ophthalmic center. A 26-year-old woman with bilateral lacrimal agenesis had epiphora and a progressive inferomedial orbital cyst. Clinical examination showed a palpable, cystic, and non-tender mass in inferomedial orbital. Lacrimal assessment showed that the lacrimal drainage pathway was congenitally absent. Orbital computed tomography (CT) confirmed the congenital absence of the lacrimal sac and nasolacrimal duct. Orbital magnetic resonance imaging (MRI) showed a well-defined inferomedial right orbital cystic lesion next to the expected lacrimal fossa region. Whole-exome sequencing did not find pathogenic variants related to lacrimal dysgenesis. The patient had CCCR under general anaesthesia using a combined external and endoscopic approach. CCCR included an external conjunctivo-canaliculo-cystic microanastomosis to establish continuity between the ocular surface outflow pathway and the cystic lumen, and an endoscopic cysto-rhinostomy to create an opening from the cystic cavity into the nasal space. Temporary bicanalicular silicone stenting was used to support maturation of the reconstructed tract. Then the stent removal, and lacrimal irrigation and nasal endoscopy were used for serial postoperative assessment. Results: CCCR was completed without intraoperative complications. After the operation, the inferomedial orbital mass and epiphora disappeared. Lacrimal irrigation showed that the reconstructed drainage pathway was patent at 2 weeks and 2 months, and it remained patent at 4 months (after stent removal). Nasal endoscopy showed a stable, epithelialised ostium without stenosis, which supported long-lasting communication between the reused cystic cavity and the nasal cavity. Histopathological evaluation of the excised cyst wall confirmed that it was a benign epithelial cyst, which was suitable as a non-malignant cystic substrate suitable for use as a new lacrimal conduit in this case. Conclusions: In a patient with congenital absence of the lacrimal sac and nasolacrimal duct complicated by an inferomedial orbital cyst, CCCR-an external conjunctivo-canaliculo-cystic microanastomosis combined with endoscopic cysto-rhinostomy and temporary bicanalicular silicone stenting-successfully restored tear outflow and resolved both epiphora and the cystic mass, with sustained patency after stent removal. CCCR offers an anatomy-sparing surgical option when conventional DCR is impossible. It also shows that it is feasible to reuse an inferomedial orbital cystic cavity as a new lacrimal conduit in carefully selected cases of congenital lacrimal drainage agenesis.
全文
HIGHLIGHTS
1. Critical Discoveries and Outcomes
• Conjunctivo-canaliculo-cysto-rhinostomy (CCCR) successfully repurposed a benign orbital cyst as a functional neo-lacrimal conduit, achieving complete resolution of epiphora and the mass with maintained patency at 4months post-stent removal.
2. Methodological Innovations
• First description of CCCR combining external conjunctivo-canaliculo-cystic microanastomosis with endoscopic cysto-rhinostomy to reconstruct tear outflow without a native lacrimal sac.
3. Prospective Applications and Future Directions
• CCCR offers a viable anatomy-sparing alternative for selected patients with congenital lacrimal agenesis and adjacent benign orbital cysts, potentially expanding the reconstructive landscape beyond conventional DCR.
The prevalence of congenital nasolacrimal duct obstruction (CNLDO) is between 5% and 20% in early childhood. CNLDO is the most common congenital tear outflow disorder and usually shows up early with epiphora.[1-2] Epiphora is not a minor problem. In a multicenter survey of 342 epiphora patients, tearing limited many daily activities. Outdoor activities were among those most seriously hindered. And post-surgical scores improved a lot. This shows the value of effective intervention for quality of life.[3] Prospective patient-reported outcome data also show significant improvement in symptoms and health-related quality of life after surgery for epiphora. This supports the clinical need to restore tear drainage when symptoms persist.[4]
In this situation, congenital lacrimal drainage anomalies are not common.[5] But they are especially challenging when the lacrimal sac and nasolacrimal duct are absent. This is because standard external or endoscopic dacryocystorhinostomy (DCR) needs a sac-to-nose anastomosis.[6-7]
Here, we report a patient. The patient has congenital absence of both the lacrimal sac and nasolacrimal duct, has no family history, and has epiphora that is made worse by an external appearance deformity. We found no similar case. We describe using a combined external and conjunctivo-canaliculo-cysto-rhinostomy (CCCR) to turn a pathological orbital cyst into a functional part of a new lacrimal system. The aim is to restore physiological tear outflow and keep good appearance.
Methods
Design, setting, and participants
This is a single-patient case report from a tertiary ophthalmic centre. A 26-year-old woman with congenital medial canthal dysplasia and bilateral agenesis of the lacrimal sac and nasolacrimal duct. She came with a 1-year history of inferomedial right orbital swelling and epiphora on the same side. Her past eye history included corrective surgery on her right eyelid and symblepharon lysis on her left eye with amniotic membrane transplantation.
Patient and diagnostic workup
The examination showed that there was a palpable, cystic mass in the inferomedial area. This mass wasn't tender, and there was no restriction of movement or visual impairment. Lacrimal irrigation showed that there was bilateral canalicular obstruction. An orbital CT scan revealed bilateral proximal bony nasolacrimal duct atresia, along with a lesion in the inferomedial right area (Figure 1A-C). An MRI scan showed a T2-hyperintense, well-circumscribed cyst, which was consistent with a benign fluid-containing structure (Figure 1D, E). Whole-exome sequencing (WES) did not find any pathogenic variants associated with lacrimal dysgenesis.
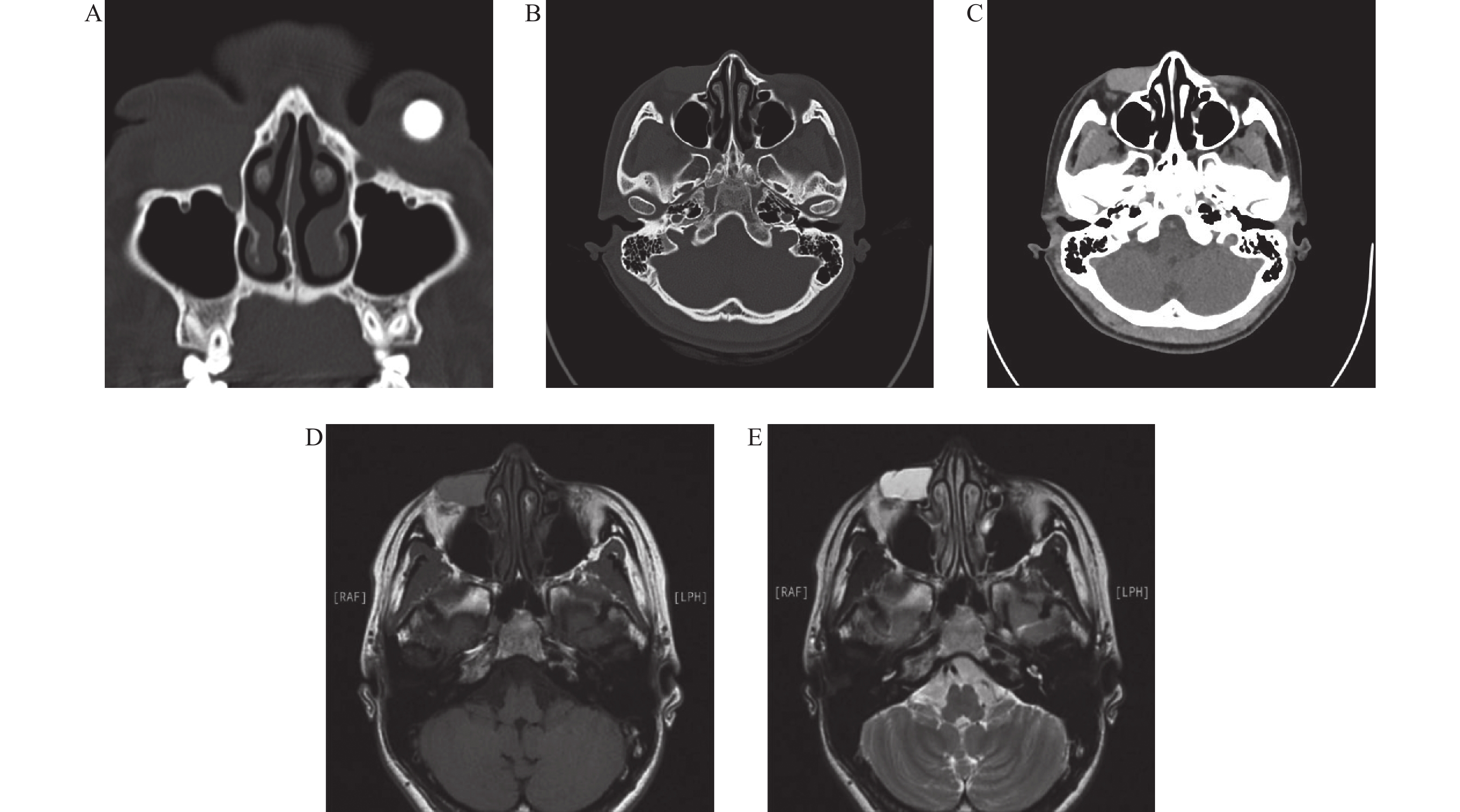
(A) Coronal computed tomography (CT) scan (bone window) demonstrating bilateral bony nasolacrimal duct atresia. (B) Axial CT scan (bone window) revealing a well-defined, oval, hyperdense mass in the subcutaneous plane of the right lower eyelid, extending from the lacrimal sac fossa. (C) Axial CT scan (soft tissue window) further delineating the homogeneous, hyperdense mass. (D) Axial T1-weighted magnetic resonance (MR) image showing a hypointense, bag-like cystic lesion in the right lacrimal sac and nasolacrimal duct region. (E) Axial T2-weighted MR image confirming the lesion as hyperintense, consistent with a fluid-filled structure.
Rationale for surgical approach selection
The choice to proceed with CCCR was made after a full assessment of the patient's special anatomical and clinical situation. The patient was born without a lacrimal sac and nasolacrimal duct, so normal dacryocystorhinostomy couldn't be done. An orbital CT and MRI confirmed there was a well-defined inferomedial orbital cystic lesion. This cyst was next to where the lacrimal fossa was expected to be and, showed benign imaging features. So, it was thought to be suitable for being turned into a new lacrimal conduit. The procedure was meant to solve two problems at once: functional epiphora and the cosmetic issue caused by the cystic mass. This case shows that CCCR can be considered for carefully chosen patients. These patients should have real lacrimal drainage agenesis and also have an adjacent, benign orbital cyst. And this cyst can be used to create a new drainage pathway.
Interventions and surgical technique
The patient was under general anaesthesia. CCCR - a combined external and endoscopic endonasal procedure - was carried out to turn the cyst into a neo-lacrimal conduit.
External step: A cut was made at the medial canthus. The cyst was found and its pressure was relieved while keeping its wall intact. Two microanastomoses were made using 8-0 sutures: 1) one was between the fornix flaps and cyst wall (conjunctive-cystic); 2) The other was made by cutting off the blocked inferior canaliculus and stitching its nasal end to the cyst wall(canaliculo-cystic).
Endoscopic step: Through the nostril, a hole was made in the bone in front of the axilla of the middle turbinate. The medial wall of the cyst was opened. A sample was taken for histopathology. Then, the cyst wall was stitched to the nearby nasal mucosa to create a cysto-rhinostomy.
Stenting and care: A bicanalicular silicone stent was put in place. Both ends of the stent came out through the nose and were tied inside the nose. Standard topical treatment and regular follow-up were given.[8] The stent was planned to be removed after 4 months. Written informed consent for publishing this case was obtained.
Results
Preoperative findings
The imaging tests confirmed that there was bilateral proximal bony nasolacrimal duct atresia and a well-defined inferomedial orbital cyst.[9] Clinical photos showed scarring on the medial lower eyelid, a 3 mm defect on the nasal side margin, and ongoing epiphora. Irrigation tests confirmed that there was canalicular obstruction on both sides.
Intraoperative and histopathology
The CCCR procedure was finished without any problems (Figure 2A-C). An endoscopic showed that there was a widely marsupialised ostium into the nasal cavity (Figure 2D). The histopathology of the removed cyst wall showed focal columnar epithelium with fibrosis underneath, which is consistent with a benign epithelial cyst (Figure 3B).[10]
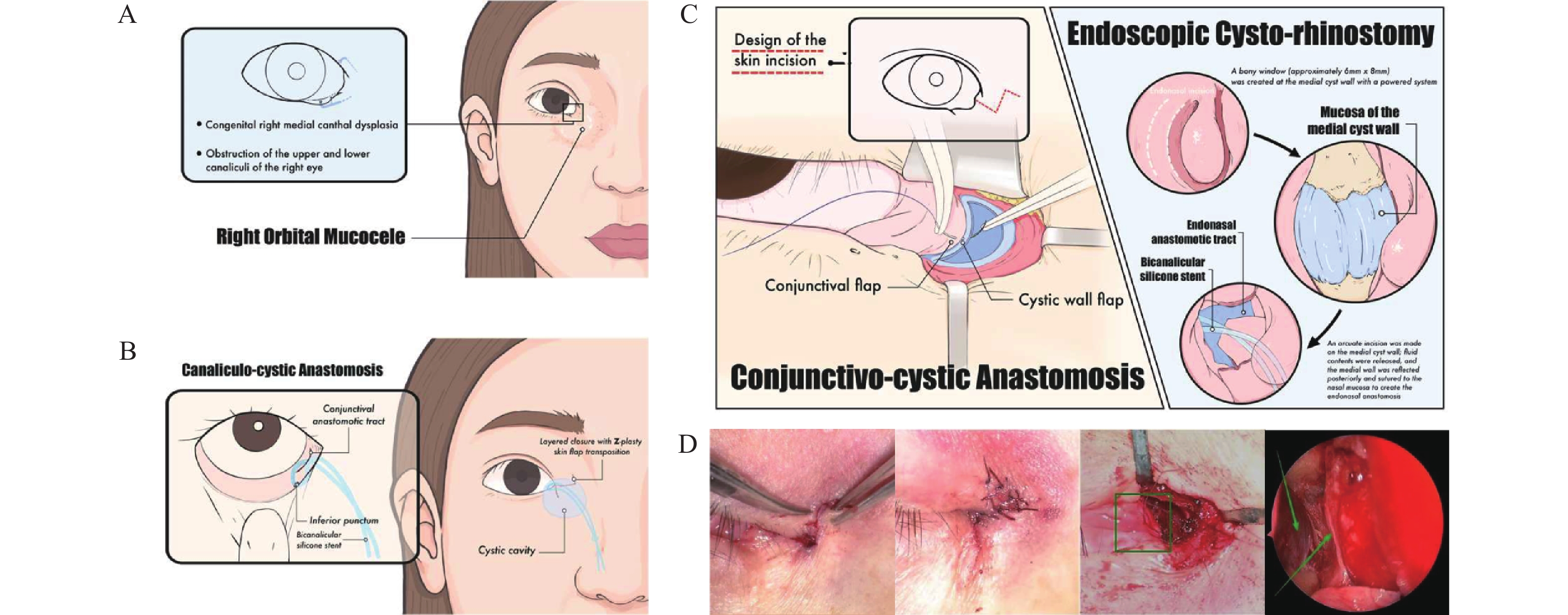
Figure A-C were hand-drawn. (A) Preoperative anatomy depicting the orbital cyst, the obstructed canaliculi and the nasal cavity. (B) The external approach illustrating the microanastomosis of the cyst wall to both the conjunctival fornix and the canaliculus. (C) Integrated overview of the completed procedure, showing the novel conduit formed by the conjunctivo-canaliculo-cystic anastomosis (external approach) and the cysto-rhinostomy (endonasal approach). (D) Intraoperative photographs depicting key surgical steps: (The left two images) Approximation of the medial canthal Z-plasty incision; (Middle) Conjunctivo-cystic anastomosis; (Right) Endoscopic view confirming the cystic marsupialization and anastomosis to the nasal mucosa (arrowhead indicates the anastomotic ostium).
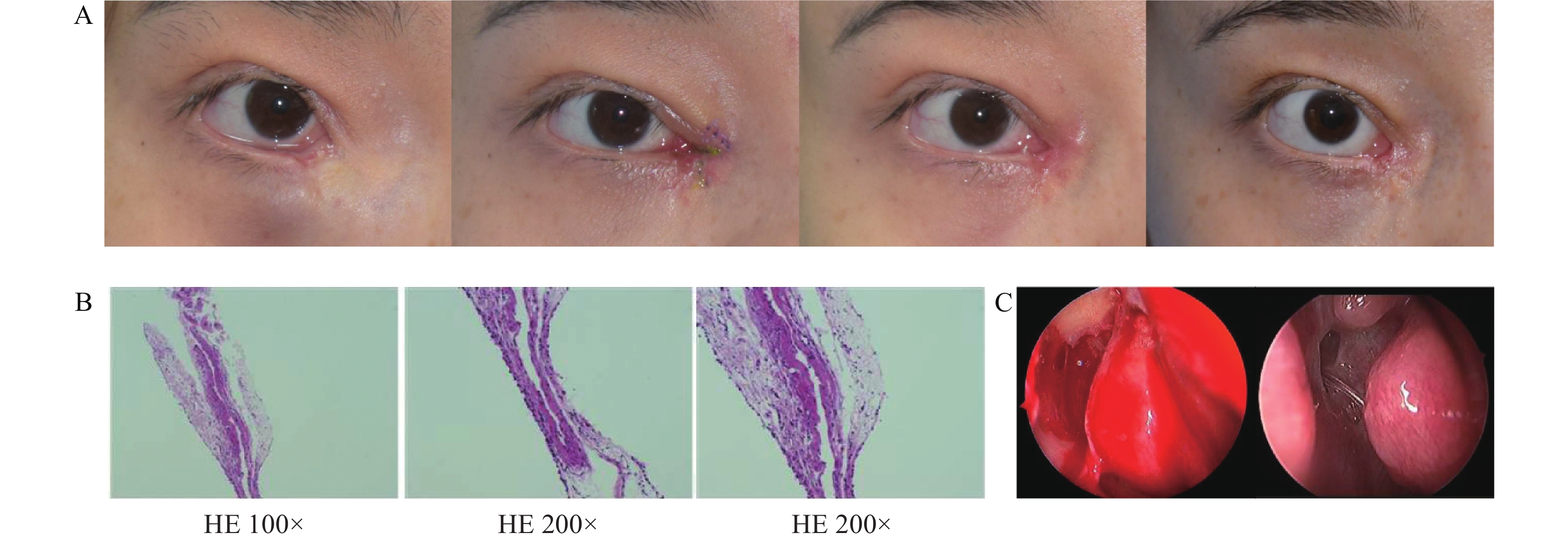
(A) Sequential clinical photographs of the right eye showing the pre-operative condition, and the post-operative appearance at 2 weeks, 2 months, and 4 months, demonstrating complete resolution of the inferomedial orbital mass and an excellent cosmetic outcome. (B) Histopathological analysis of the excised cyst wall (hematoxylin-eosin stain) reveals fibrous tissue hyperplasia and degeneration in the cyst wall. (C) Intraoperative endoscopic view showing the initial marsupialization of the cyst into the nasal cavity (left). Follow-up endoscopy at 2 months (right) confirms a well-epithelialized, patent anastomotic ostium, with the silicone stent in situ.
Postoperative course and outcomes
At 2 weeks and 2 months after the operation, the mass and epiphora had gone away (Figure 3A). Irrigation was unobstructed, and nasal endoscopy showed a well-epithelialised fistula without inflammation or narrowing (Figure 3C). After the bicanalicular stent removal at 4 months, the patency was maintained, and the appearance remained good. No bad events happened during follow-up.
Discussion
Congenital epiphora is most often caused by CNLDO, which is usually related to a membranous blockage at the valve of Hasner. Recent practice guidelines and contemporary reviews suggest a step-by-step approach: start with conservative care (e.g., Crigler massage and keeping things clean, and use antibiotics only for infections). Then, do a procedure if the blockage keeps causing symptoms or leads to complications.[11–13]
If symptoms continue after infancy, probing the nasolacrimal duct is usually the first procedure done. If that fails, repeat probing, silicone intubation (either monocanalicular or bicanalicular), or balloon dacryoplasty can be tried.[14-15] A systematic review and meta-analysis found that silicone tube intubation was more successful than probing and worked as well as balloon dilation. Monocanalicular systems were associated with fewer complications than bicanalicular intubation.[16] For stubborn blockages, especially in older children, or when anatomy is complex, DCR can create a new opening between the lacrimal sac and the nasal cavity to provide a lasting bypass.[17] Recent pediatric studies with long follow-up show that endonasal endoscopic DCR is safe and effective, with high satisfaction. But there are limits, like tube extrusion, the need for revision surgery, and lower success in children with craniofacial abnormalities or proximal lacrimal problems. This shows the importance of multidisciplinary planning when anatomy is complex.[18-19]
Besides blockages at the level of Hasner, congenital lacrimal drainage problems can include punctal or canalicular dysgenesis and agenesis, congenital fistulas, diverticula, and distal cystic lesions. These can occur alone or be part of a systemic syndromic syndrome. Treatment depends on the anatomy: reconstruction may be possible if canalicular tissue is present, but complete absence of proximal outflow often requires lacrimal bypass, which means long-term tube care and risks of migration, extrusion, or blockage.[20–24]
These data show that lacrimal surgery has evolved from minimally invasive canalicular procedures to endonasal endoscopic bypass. But there is key limit: most treatment plans assume there is a lacrimal sac and a reconstructible outflow tract. When that is not the case, like in true congenital agenesis of the lacrimal sac and nasolacrimal duct, conventional DCR is not possible. That's when a tailored, anatomy-based reconstruction is needed.[6,7,25] This case shows that CCCR can use an orbital cyst to create a continuous, epithelialised conduit from ocular surface to the nose by combining external conjunctivo-/canaliculo-cystic microanastomoses with endoscopic cysto-rhinostomy. Unlike simple cyst excision which removes the mass but gives up any chance of physiological drainage, CCCR addresses both function and appearance in one step and avoids an indwelling glass tube.
In this case, figuring out the nature and origin of the “orbital cyst” is clinically important but hard to do with just one case. The patient developed a gradually worsening inferomedial orbital swelling over about a year, which is not the typical for classic congenital dacryocystocele in infancy. Histopathology showed cyst-wall-like tissue with focal columnar epithelium and fibrous growth, supporting an epithelial-lined cyst but giving little information about where it came from. Given its location near the lacrimal fossa and the overall imaging and intraoperative findings, a lacrimal-system-related remnant remains is a possible explanation. It might have becoming clinically obvious later due to secretion retention, local inflammation, or altered outflow dynamics. Overall, the overall clinicoradiologic context suggests a lacrimal-system-related lesion, but other mucosa-derived possiblities are also in the differential diagnosis. Other causes should also be considered, like a paranasal sinus-related mucocele with orbital extension or an acquired implantation/inclusion cyst possibly related to prior eyelid surgery. Since the available clinical-pathological evidence cannot definitively determine the tissue of origin, we use descriptive terms (inferomedial orbital epithelial-lined cyst adjacent to the lacrimal fossa) and frame the cause as a differential diagnosis rather than a conclusion.
Early results-complete symptom resolution, lasting irrigation patency after stent removal, and a stable endoscopic appearance-support the technical soundness of the procedure. Practical considerations include keeping the cyst wall intact, ensuring adequate nasal ostium formation with mucosa-to-cyst contact to promote epithelialisation, and maintaining temporary stenting to prevent restenosis. WES did not find a pathogenic cause for lacrimal dysgenesis in this patient but identified a ZNF469 variant of uncertain significance, a gene involved in corneal integrity.[26-27] This incidental finding suggests the need for longitudinal corneal surveillance but is not related to the drainage reconstruction. Limits of this study include the single-case design, short follow-up, lack of fluorescein-based tear drainage assessment, and the need for coordinated oculoplastic and endoscopic expertise. Nevertheless, CCCR may be a useful option when standard anatomy is absent or severely disrupted.
Correction notice
None
Acknowledgements
The authors would like to thank the entire medical and nursing staff of the Department of Oculoplastic and Lacrimal Surgery at Zhongshan Ophthalmic Center for their dedication and expertise in managing this case.
Author contributions
(I) Conception and design: Rongxin Chen, Chengzhen Gong
(II) Administrative support: Rongxin Chen, Xuanwei Liang
(III) Provision of study materials or patients: Rongxin Chen, Xinran Dong
(IV) Collection and assembly of data: Chengzhen Gong, Xinran Dong
(V) Data analysis and interpretation: Jiayi Sun, Chengzhen Gong
(VI) Manuscript writing: All authors
(VII) Final approval of manuscript: All authors
Conflict of interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form.
Patient consent for publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of the Zhongshan Ophthalmic Center, Sun Yat - sen University, China (2025KYPJ074).
Data availability statement
None
Open access
This is an Open Access article distributed in accordance with the Creative Commons AttributionNonCommercial - NoDerivs 4.0 International License (CC BY–NC-ND 4.0), which permits the non - commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license).
基金
1. This work was supported by the Research Funds of the State Key Laboratory of Ophthalmology (2025QNJS31) and National Natural Science Foundation of China (82571265).