Utilizing a lacrimal probe for the removal of broken and dislodged silicone tubing: a case report
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
摘要
Lacrimal passage intubation is widely used to treat lacrimal system disorders. A common postoperative complication is silicone tube breakage and dislodgement. This often happens because of poor care or non-standardized removal techniques. It is especially difficult when a bicanalicular silicone tube breaks during removal and cannot be located at the nasolacrimal duct opening. We report a case that a fractured bicanalicular silicone tube remnant, which was caused by improper removal at a local hospital, was successfully taken out using a lacrimal probe. This case shows that a lacrimal probe can be effectively used to help remove a fractured bicanalicular silicone tube that stays inside the lacrimal duct.
全文
HIGHLIGHTS
1. Critical Discoveries and Outcomes
• Even when a fractured silicone tube retracts deep into the lacrimal system and is invisible in the nasal cavity, the remaining stump can serve as a natural conduit for intervention. Using this method, the fractured tube was completely removed without any iatrogenic damage to the puncta, mucosa, or lacrimal duct, completely avoiding the trauma associated with surgical incision.
2. Methodological Innovations
• Introduction of the “probe-guided intraluminal push-out technique.” By utilizing the residual tube stump as a natural guide, a lubricated lacrimal probe is inserted retrograde into the lumen to push the retracted distal knot directly into the nasal cavity. This technique both reduces the risk of re-fracture and achieves a minimally invasive extraction.
3. Prospective Applications and Future Directions
• This simple and cost-effective technique is particularly suitable for promotion in primary care hospitals, providing a reference for managing retained fractured silicone tubes after lacrimal intubation.
• Multicenter studies are needed to validate its generalizability. Additionally, efforts should focus on optimizing instrument design—developing specialized intraluminal retrieval devices—and promoting standardized postoperative protocols for managing tube fractures.
Bicanalicular silicone tubes are widely used in lacrimal duct intubation for obstructive disorders and for the anastomosis of lacrimal duct disruptions.[1] The bicanalicular silicone tube is passed one after another through the lacrimal punctum, canaliculus, lacrimal sac, and nasolacrimal duct to reach the inferior nasal meatus. Then, the free ends are knotted and placed.[2] This keeps the new channel open, helps tear drain, and reduces anastomotic scarring and stenosis.[3]
Silicone tube breakage is a common problem. It often happens because of poor postoperative care or wrong removal methods.[4] When the tube breaks, the distal tube part and knot often go back into the nasolacrimal duct or lacrimal sac.[3] This makes it hard to find the remaining tube part using normal probing methods through the lower nasal passage or nasolacrimal duct opening. Consequently, it is very difficult to safely remove the remaining silicone tube in the lacrimal duct.
This report describes a novel technique. It uses a lacrimal probe to successfully get out such fractured and retained bicanalicular silicone tubes.
Case presentation
A patient got a right lower eyelid cut and a tear in the inferior canaliculus from a steel pipe injury in August 2024. A local hospital did a surgical anastomosis and put in a bicanalicular silicone tube. The patient recovered well. When trying to take out the tube in November 2024, excessive force made the tube break. We could see the remain part of the silicone tube at the upper lacrimal punctum, but we didn’t see any tube at the lower lacrimal punctum (Figure 1A). Both the upper and lower lacrimal punctums were still in good shape. And we couldn't clearly see the tube in the lower nasal passage or at the nasolacrimal duct opening (Figure 1B). This made it hard to remove the tube, so the patient was sent to our hospital.
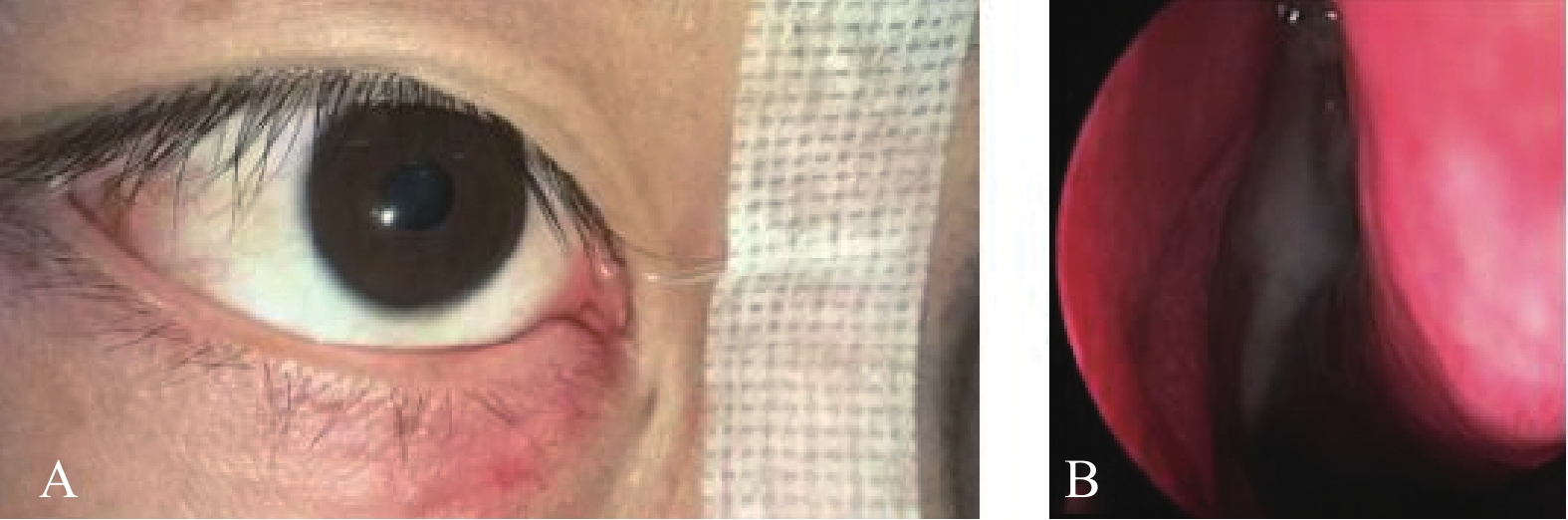
(A) Surgical scar on right lower eyelid. Silicone tube remnant (~3 cm) visible at upper punctum (trimmed excess); no tube at lower punctum. (B) Distal tube segment and knot buckle retracted into nasolacrimal duct/lacrimal sac. Tube not clearly visible in inferior meatus or at nasolacrimal opening.
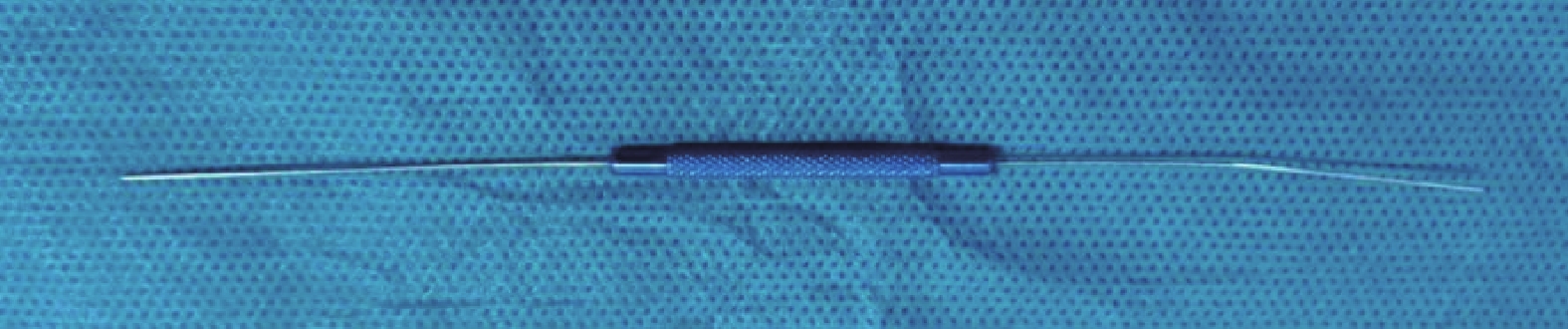
Considering the patient’s situation, we planned to use a lacrimal probe (Figure 2) to remove the retained tube. And we would use nasal endoscopy to guide the process. There is a diagram that shows the procedure (Figure 3).
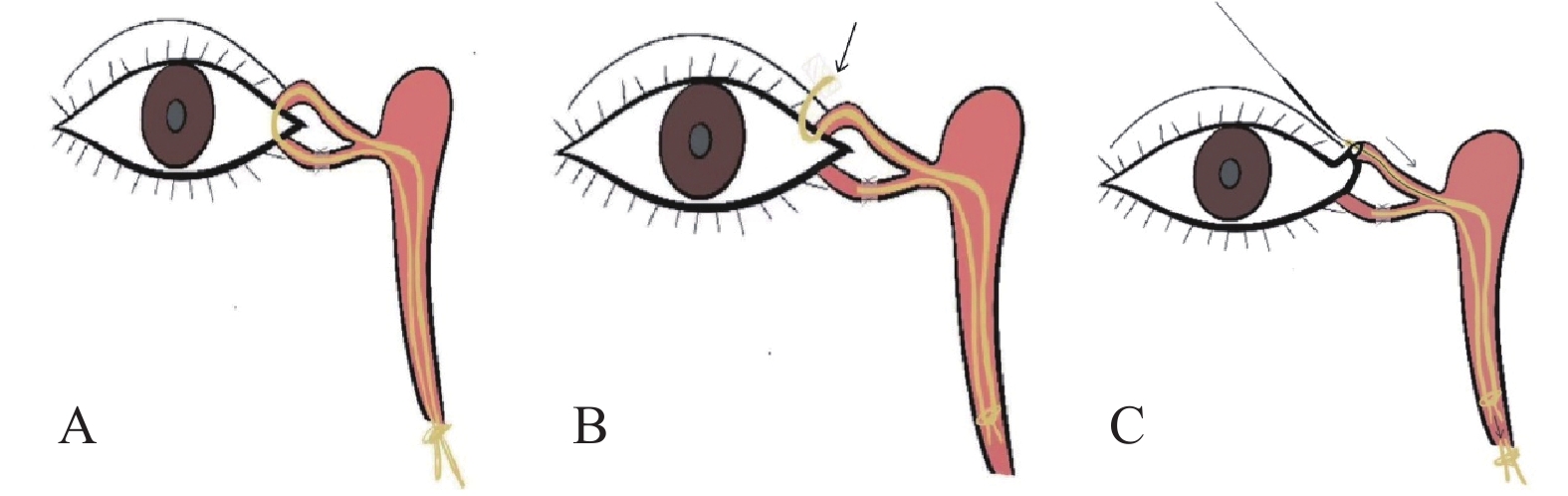
(A) Normal tube fixation pre-breakage. (B) Tube fractured, stump visible only at upper punctum. (C) Probe inserted via upper punctum stump ejects tube into the inferior nasal passage.
Here are the detailed surgical steps (Figure 4): 1) The patients laid on their back. After disinfecting the surgical area, we used promethazine eye drops for surface anesthesia. We put cotton pads soaked in a 0.01% epinephrine lidocaine solution into the inferior nasal tract for two minutes to make the nasal mucosa shrink. 2) We found the opening of the silicone tube stump in the upper lacrimal punctum. We lubricated the tip of a No. 5 lacrimal probe with recombinant bovine alkaline fibroblast growth factor gel (Figure 4A). Then we carefully inserted the probe through the opening of the stump in the upper lacrimal punctum and pushed it to the knot (Figure 4B). 3) We inserted the lacrimal probe, along with the stump of the silicone tube, into the lacrimal canal through the upper lacrimal punctum. Then we slowly moved it through the lacrimal punctum, lacrimal canal, lacrimal sac, and nasolacrimal canaliculus to reach the lower nasal passage (Figure 4C). 4) After the lacrimal probe pushed the silicone tube out of the nasolacrimal duct, as we could see through nasal endoscopy (Figure 4D), we put a diagonal hook into the lower nasal canaliculus to catch the silicone tube (Figure 4E). Then we pulled, the silicone tube out through the front of the nose (Figure 4F). 5) Then we used gun forceps to hold the fixed silicone tube knot buckle inside in the front of the nostril. At the same time, we carefully pulled the lacrimal probe out of the upper punctum in the opposite direction (Figure 4G). It is crucial to make sure that the probe doesn't accidentally pull the silicone tube out of the upper lacrimal punctum during this step. 6) We gently pulled the remaining silicone tube in the lacrimal duct out through the front of nostril (Figure 4H), and checked that the silicone tube was complete (Figure 4I). We did the surgery carefully to avoid any further damage to the silicone tube.
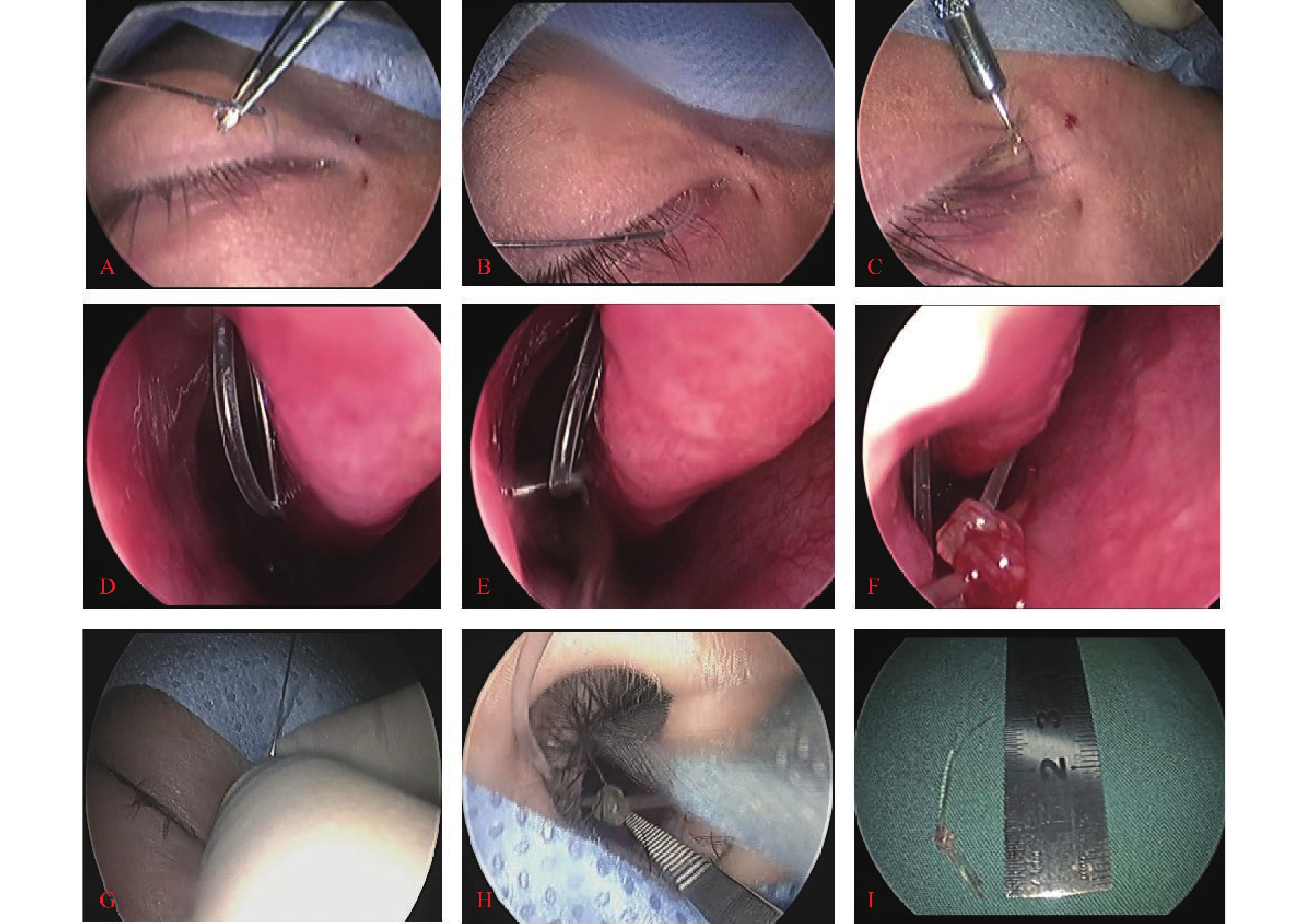
(A) Insert lubricated probe into tube stump at upper punctum. (B) Push the lacrimal probe to the knot. (C) Navigate the lacrimal probe into the lacrimal duct from the upper lacrimal punctum. (D) Probe displaces tube into the inferior nasal passage. (E) Extract the silicone tube using a diagonal hook. (F) Extract tube through naris. (G) Withdraw probe from the upper lacrimal punctum. (H) Remove the fragmented silicone tube from nostril. (I) Confirm tube integrity.
The operation was a success. The remaining piece of the silicone tube was completely taken out, and there was no damage to surrounding structures (like the puncta, mucosa, skin) (Figure 5). The patient was discharged with no problems after surgery.

Discussion
Bicanalicular silicone intubation is often used in lacrimal surgery.[1-2] After surgery, the tube can break. This may happen because the silicone gets old, the knot is tied too tight, the patient rubs their eye, or the tube is removed improperly.[3] It is usually hard to see where the remaining pieces are, which makes taking them out difficult.[5] This case shows how hard it is to deal with tube fractures when there is only a stump in one punctum and nothing can be seen in the nose. If we try to pull the tube out forcefully, it may break again and damage the canaliculi, sac, or duct. This could lead to infection, the duct getting narrow again, or the pump function being impaired. Doing surgery through a skin cut or using nasolacrimal endoscopy can cause more trauma and scarring. In this case, we successfully got the remaining piece out through its original path using a lacrimal probe under endoscopic guidance, avoiding complications.
There are still some important things to pay attention to when using this method in practice: First, because the silicone tube has a narrow lumen, we chose a No. 5 lacrimal probe. We put get on it before inserting it to make it easier to pass through and reduce the risk of tearing the lumen. Second, when putting the lacrimal probe and the silicone tube stump into the tear duct, we should do it gently. If there is any resistance, we could not force it to avoid creating a false tunnel. Third, when pulling out the lacrimal probe, it is very important to hold the silicone tube stump at the inner corner of the eye and pull the silicone tube back into the tear duct when removing the probe. Just holding the silicone tube at the front of the nose is not enough, because this may cause it to break again when pulling. Fourth, after taking it out, we should check the silicone tube carefully to make sure there are no remaining pieces in the tear duct.
Previous studies have also described using a lacrimal probe to move dislocated silicone tubes back through the lumen.[6] Compared with this method, our approach focuses on solving the problem of dislocation after silicone tube intubation. If the silicone tube is still intact and needs to be put back in place, we should try to move it. On the other hand, if the tube is broken, we should try to get it out.
This complication does not happen often, so our sample size is small. More studies are needed to check the safety of this method and possible complications. Being gentle is very important. If we use too much force, the tube may break again or the probe may come off, leaving the tube completely inside and requiring surgical removal.
Furthermore, in future clinical practice, we must give patients better postoperative care instructions (such as avoiding eye rubbing, not blowing the nose hard, and closing the eyes when washing). Clinicians should be careful when removing tubes and choose the right method according to the type of tube instead of using forceful removal methods. Taking these measures can greatly reduce the risk of postoperative silicone tube breakage.
Conclusion
We successfully took out a broken bicanalicular silicone tube that was stuck in the lacrimal system. We used a lacrimal probe and nasal endoscopy to guide us. This method is simple, safe, reliable, and cost-effective It provides a good way to deal with this difficult problem.
Correction notice
None
Acknowledgements
None
Author contributions
(I) Conception and design: Xuanwei Liang, Rongxin Chen
(II) Administrative support: Xuanwei Liang
(III) Provision of study materials or patients: Xuanwei Liang
(IV) Collection and assembly of data: Xinyu Zheng, Yuanxia Yang
(V) Data analysis and interpretation: Xinyu Zheng, Xinyue Yu
(VI) Manuscript writing: All authors
(VII) Final approval of manuscript: All authors
Conflict of interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form.
Patient consent for publication
None
Ethical statement
This study was approved by the Institutional Review Board of the Zhongshan Ophthalmic Center, Sun Yat-sen University, China (2021KYPJ100) and adhered to the tenets of the Declaration of Helsinki.
Data sharing statement
None
Open access statement
This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license).
Supplementary materials
基金
1. This work is supported by the Natural Science Foundation of Guangdong Province of China (2021A1515012043).