


HIGHLIGHTS
• Analysis of the current domestic and international status of diagnosis and treatment of bloody tears reveals complex etiology and non-standardized management approaches, with a lack of systematic diagnostic and treatment guidelines both in China and internationally.
• The etiology and clinical manifestations of bloody tears are diverse and complex, often involving multiple disciplines and specialties.
• Different causes of bloody tears exhibit significant variations in both clinical presentations and treatment methodologies.
• This expert consensus systematizes the clinical characteristics and etiologies of bloody tears, establishing diagnosis and treatment protocols to guide clinicians in the proper management of patients with this condition.
Bloody tears, also known as haemolacria, are a symptom characterized by blood-tinged tears flowing from the eye, which can be caused by a variety of factors. Patients may present with overt ocular hemorrhage, concealed bloody tears, or blood-tinged secretions.[1-2] In recent years, there has been an increase in literature reports on bloody tears, and it also seems that the number of patients presenting with this symptom is on the rise.[1-4] The etiology and clinical manifestations of bloody tears are complex and multifaceted, often requiring the collaboration of multiple medical disciplines and specialties. Diagnostic and therapeutic strategies can vary significantly depending on the underlying etiology.[1-4] Historically, there has been a notable lack of comprehensive and systematic understanding of this condition. Most of the existing literature consists of case reports, and there is a conspicuous absence of standardized diagnostic and treatment protocols. This lack of established guidelines may leave healthcare professionals, especially those working in emergency settings who encounter patients with severe bloody tears, without sufficient guidance.
To provide clinicians with a standardized and referenceable framework for the clinical diagnosis and treatment of bloody tears, the Lacrimal Diseases Professional Committee of the Ophthalmologist Branch of the Chinese Medical Doctor Association, along with the Lacrimal Diseases Group of the Ophthalmic Professional Committee of the Chinese Association of Integrated Medicine, convened a panel of relevant experts. This consensus is based on the combined clinical experiences of the experts and a thorough review of both domestic and international research related to bloody tears. Its objective is to offer guiding recommendations regarding its etiology, clinical manifestations, and management strategies of bloody tears.
Methodology of consensus development
The establishment of this expert consensus was initiated and coordinated by two key organizations: the Lacrimal Diseases Professional Committee of the Ophthalmologist Branch of the Chinese Medical Doctor Association and the Lacrimal Diseases Group of the Ophthalmic Professional Committee of the Chinese Association of Integrated Medicine. To this end, a panel of experts was assembled, predominantly comprising specialists in lacrimal diseases and related ophthalmological fields from different regions across China.
The consensus was formulated based on two main foundations. One is the "clinical practice experience" accumulated by these experts over the years, and the other is a comprehensive "summary of domestic and international research on the diagnosis and treatment of bloody tears." Throughout the process, strict adherence was paid to "standardized procedures for establishing consensus", as reference in the source document.[5-6]
These standardized procedures cover a series of steps. They include conducting systematic literature reviews to gather relevant information, holding several rounds of expert discussions and deliberations to exchange ideas and insights, evaluating the available evidence to assess its quality and applicability, and iterative refining the statements until a consensus is reached. It is worth noting that, given the significant emphasis placed on "clinical practice experience," expert opinion played a particularly crucial role in areas where high-quality evidence from randomized controlled trials are in short supply. After in-depth discussions and multiple rounds of revisions, the expert panel successfully formulated guiding opinions on the etiology, clinical characteristics, as well as the diagnostic and treatment procedures for bloody tears. The ultimate goal is to provide clinicians with a practical and systematic framework to effectively manage this condition.
Etiology of bloody tears (Haemolacria)
The origin of bloody tears can be traced back to the eyeball itself, the ocular adnexa (which encompasses the eyelids, lacrimal apparatus, conjunctiva), or even the nasal cavity. The potential causes of bloody tears are extensive and highly diverse, spanning a wide spectrum that includes inflammation, tumors, trauma, surgical complications, coagulation disorders, vascular anomalies, abnormalities of the mucous membranes, psychological factors, drug-related side effects, as well as idiopathic conditions. A summary of common causes is presented in Table 1.
|
Category |
Specific Area/Condition |
Examples/Details |
|
Local causes |
Lesions or injuries of the ocular surface and surrounding tissues |
|
|
Lesions and injuries of the lacrimal drainage system and surrounding tissues |
|
|
|
Other local pathological conditions |
Cranial base fractures, ocular/lacrimal endometriosis, hormonal sensitivity, mucosal hypersensitivity to irritants |
|
|
Systemic disease-related causes |
Coagulation disorders |
|
|
Vascular morphological and functional abnormalities |
|
|
|
Other systemic diseases |
Hypertension, thyroid dysfunction, diabetes mellitus, renal failure |
|
|
Other special causes |
Drug-related Factitious causes Psychogenic and psychological Factors Idiopathic haemolacria |
Local causes
Lesions or injuries of the ocular surface and surrounding tissues
The anatomical regions that can be implicated in the occurrence of bloody tears include the eyelids, lacrimal gland, conjunctiva, and sclera. Pathologies affecting the eyelid, such as eyelid diseases, injuries, or parasitic infestations, as well as conditions involving the sclera, have the potential to result in bloody tears.[7-11] Diseases of the lacrimal gland can disrupt the blood-tear barrier, enhance vascular permeability, or directly cause damage to the lacrimal tissue or its vascular structures, thereby leading to haemolacria. Conjunctival lesions and injuries rank among the most prevalent causes of bloody tears. These often have identifiable etiologies, including foreign bodies, inflammation conditions (for instance, conjunctivitis), or tumors (such as conjunctival melanoma).[7] Such factors can include damage to the conjunctiva or even lead to its invasion.[1,7,12-20]
Lesions and injuries of the lacrimal drainage system and surrounding tissues
This category encompasses pathologies affecting the lacrimal system (including canaliculi, lacrimal sac, nasolacrimal duct), nasal cavity, paranasal sinuses, and orbit. Among these, lesions and injuries of the lacrimal drainage system are the most common cause of severe bloody tears. When there is spontaneous bloody reflux from the lacrimal passage, it should prompt suspicion of tumors, especially malignant ones.[1,21-30]
Benign conditions can also give rise to bloody tears. These include inflammatory lesions, tuberculosis, granulomas, foreign bodies, iatrogenic injuries, hemangiomas, varices, and papillomas.[1,24,26,31-44] Idiopathic bloody tears often have their origin in the lacrimal drainage system. Nasal trauma or procedures such as nasal packing can induce retrograde blood flow into the nasolacrimal duct and lacrimal sac, which then exits through the puncta.[45-48]
Nasal fractures may also involve the lacrimal duct, resulting in retrograde bleeding from the puncta. This bleeding may be accompanied by epistaxis.[49] Inflammatory or other lesions in the nasal cavity can extend to the nasolacrimal duct and sac, leading to bloody tears.[37,50] Pathologies or foreign bodies in the maxillary sinus, ethmoid sinus, or orbit can invade the lacrimal system, causing bloody reflux from the puncta.[35,50-52] Bloody tears resulting from these causes may sometimes be accompanied by epistaxis as well.
Other local pathological conditions
Cranial base fractures may lead to the leakage of cerebrospinal fluid and blood into the conjunctival sac or nasal cavity, and this leakage can occasionally present as bloody tears. Additionally, ocular or lacrimal endometriosis may give rise to the occurrence of bloody tears. These tears may coincide with the menstrual cycle; in some instances, they may manifest as regular yet non-cyclical bleeding.[53-55]
The conjunctiva is also sensitive to hormonal fluctuations, such as those related to estrogen-induced premenstrual hypertension. Such hormonal changes may result in the development of bloody tears.[56] Moreover, hypersensitivity of the ocular or lacrimal mucosa to irritants, including irritant gases and intense light, among others, can increase vascular permeability. This, in turn, leads to the appearance of bloody tears, which are characterized by diffuse conjunctival oozing.[57-58] These bloody tears may potentially be accompanied by bleeding from other anatomical sites.[59]
Systemic disease-related causes
Bloody tears may present either in isolation or simultaneously with other types of hemorrhage, including hematohidrosis (bloody sweat), epistaxis, purpura, gastrointestinal bleeding, and so on. In such cases, bloody tears serve as an ocular sign indicating an underlying systemic disorder.
Coagulation disorders
Certain hematological or immunological disorders can give rise to deficiencies in clotting factors or thrombocytopenia. These conditions disrupt the normal coagulation process, thereby leading to the appearance of bloody tears.[60-64] Moreover, the long-term administration of anticoagulant medications may also induce comparable effects, which in turn contribute to the occurrence of bloody tears.[65]
Vascular morphological and functional abnormalities
Abnormal capillaries, which are often fragile, have a high propensity to rupture. When these abnormal capillaries are located in ocular or lacrimal tissues, they may rupture in response to certain stimuli, ultimately resulting in the occurrence of bloody tears. Typical examples of such abnormal capillaries include telangiectasis, hemangiomas, and varices.[1,15,41,66-68] Certain conditions can elevate vascular permeability, thereby leading to the development of bloody tears. These conditions encompass allergic purpura, drug-induced rashes, vasculitis, erythema multiforme-like drug eruptions, and acute hemorrhagic edema.[59,69-70] Additionally, a deficiency of vitamin C can also increase vascular permeability and subsequently cause bloody tears.[71]
Other systemic diseases
Severe and inadequately controlled hypertension has the potential to trigger or exacerbate the occurrence of bloody tears.[51,72-73]. Additionally, thyroid dysfunction has been linked to bloody tears,[74] owing to its association with coagulation disorders or increased vascular permeability. Diabetes mellitus can induce vascular endothelial damage, while renal failure can result in hemolytic anemia, platelet dysfunction, and coagulopathy. These systemic diseases may all be correlated with the occurrence of bloody tears.
Systemic diseases can independently give rise to the occurrence of blood tears, or they can function as contributing factors that intensify the occurrence of this condition. In some cases, blood tears may be associated with the simultaneous presence of multiple systemic diseases.[75]
Other special causes
Drug-related
Methacholine and acetylcholine have the potential to induce vasodilation, which may subsequently lead to the appearance of bloody tears.[2]
Factitious causes (e.g., Munchausen syndrome)
Individuals may insert foreign objects into the conjunctival sac or self-inflict conjunctival injuries, resulting in bloody tears. Such patients may feign or provoke illness in an attempt to gain sympathy, care, or exert control. This behavior often indicates the presence of an underlying psychological disorder and may be accompanied by other atypical behaviors.[1,34,76-78]
Psychogenic and psychological factors
Mental and psychological factors can act as triggers for bloody tears.[79-83] The proposed mechanism is as follows: psychological stress can cause vasoconstriction through the stimulation of adrenaline. Once the stress is relieved, excessive vasodilation may occur, potentially reaching the point of rupture. Alternatively, changes in vascular permeability and extravasation of blood can also take place. These physiological changes can manifest as bloody tears, hematohidrosis, gastrointestinal bleeding, or bleeding from multiple sites.[80-81] Gardner-Diamond syndrome (also known as autoerythrocyte sensitization syndrome, or psychogenic purpura) can also cause bloody tears and is associated with significant stress, possibly accompanied by headache, dizziness, fatigue, and diplopia.[84] Munchausen syndrome, mentioned earlier, also falls under this category.[34,77-78]
Idiopathic haemolacria
This condition usually occurs in adolescents, with a slight female predominance. The cause of the bleeding remains unknown, and the condition is typically self-limiting. Occasionally, it may be accompanied by bleeding in other sites, such as hematohidrosis, epistaxis, tympanic membrane bleeding, and scalp bleeding. Some researchers have proposed a possible connection to psychological factors.[1,85-96]
Clinical features of bloody tears
Bloody tears can present either as an isolated clinical symptom or in conjunction with other clinical manifestations. They may occur unilaterally or bilaterally, either simultaneously or sequentially, and could be associated with bleeding from other anatomical locations. A unilateral occurrence typically indicates localized pathology, whereas bilateral involvement or simultaneous bleeding from other regions generally suggests systemic disorders or alternative etiological factors. The presence of concurrent abnormal behaviors may imply the influence of psychogenic factors.
The appearance of bloody tears can vary widely, ranging from thin, blood-tinged fluid to bloody discharge, or even fresh blood. Some cases are subtle and easily go unnoticed, while others are severe. Then, bloody tears usually suggest lesions in the tissues surrounding the tear lake. Bloody discharge is commonly observed in systemic diseases that involve the lacrimal drainage system, especially when accompanied by purulence. The presence of fresh blood often indicates the possibility of vascular rupture or malignant lesions. Bloody tears with clear triggers, such as exposure to irritant fumes or gases, suggest a possible link to increased vascular permeability. In female patients, the occurrence of bloody tears may occasionally be cyclical, either in sync or out of sync with menstruation, typically pointing to endometriosis. In adolescents, after organic pathology has been ruled out, psychogenic or idiopathic haemolacria should be considered.
Bloody tears may be accompanied by other symptoms, including epistaxis, epiphora, purulent discharge, a mass in the lacrimal sac region, or decreased vision. Bloody tears associated with systemic diseases often present with bleeding or purpura at other sites, which may be in visible locations or occult (e.g., intracranial hemorrhage, gastrointestinal bleeding). Depending on the location of the associated pathology, patients may experience other symptoms such as headaches or abdominal pain.
Diagnostic workup and procedures
A systematic approach is of vital importance for diagnosing the causes of bloody tears. The diagnostic process entails taking a careful medical history, conducting a thorough physical examination, and performing targeted investigations, all of which are guided by the patients’ clinical presentation and the suspected etiology. The diagnostic and treatment flowchart (Figure 1) has been specifically designed to aid clinicians in carrying out this process.
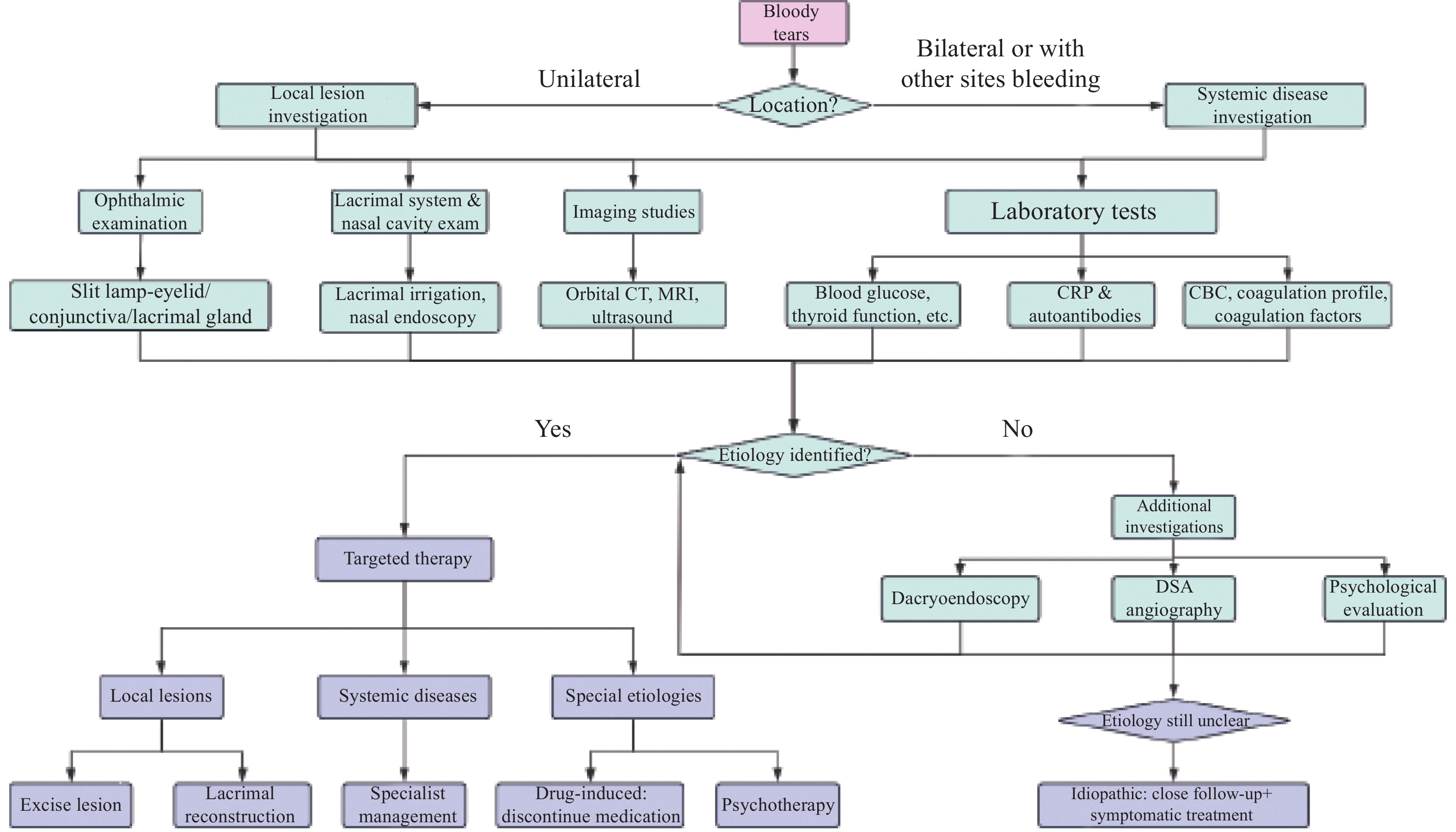
Figure 1 from the original consensus document, illustrating the proposed diagnostic and treatment pathway for bloody tears.
Patient demographics and comprehensive history
Collect patient demographic information. Obtaining a detailed medical history is utmost importance, and it should cover the following aspects:
• Characteristics of bloody tears: Identify the affected eye(s), describe the nature of the bleeding (e.g.,whether it is tinged or frank blood), and note the frequency and periodicity of the bleeding episodes.
• Associated symptoms: Look for ocular symptoms such as pain, itching, and diplopia. Also, be alert to systemic discomfort, including abdominal pain or headache.
• Triggers and modifying factors: Determine any known triggers that may have precipitated the bleeding episodes.
• Past medical and surgical history: Inquire about the patient’s previous medication use, surgical procedures, history of head or facial trauma (especially involving the ocular or nasal), and exposure to foreign bodies.
• Family history: Pay particular attention to any history of bleeding disorders within the family.
• Social and environmental history: Assess the patient’s living environment, taking into account both physical and psychosocial factors, as well as their mental and psychological state.
• Systemic bleeding: Specifically ask about bleeding or purpura from other sites in the body.
Patients should be encouraged to document their bleeding episodes by taking photos or videos, which can provide valuable visual evidence for diagnosis. For some individuals, long-term follow-up may be necessary to monitor their condition. During consultations, clinicians should observe patients for any abnormal behavior or speech patterns and inquire about significant life events or stressors that may be contributing to their condition. If necessary, family members can be involved to provide collateral information that may aid in the diagnostic process.
Physical examination
Ophthalmological examination
• Routine examination: Visual acuity, intraocular pressure, refraction, and fundoscopy.
• Slit-lamp examination: A thorough and detailed examination should be conducted on the lacrimal gland, eyelids, conjunctiva, and puncta to detect the presence of foreign bodies, masses, or signs of trauma. Palpation of the lacrimal sac area is also essential to check for reflux, which can assist in determining the source and cause of bleeding. It is important to always perform a bilateral comparison during the examination to ensure comprehensive assessment. Additionally, clinicians should check for any palpable masses or areas of tenderness in the medial canthal region or orbit.
• Specific tests for suspected lacrimal system bleeding: When bleeding from the lacrimal system is suspected, a punctal plug can be inserted. This allows for a clearer observation of the bleeding site.[97] Ideally, the examination should be carried out during an active bleeding episode to obtain the most accurate information. However, if active hemorrhaging is not present, employing the Valsalva maneuver may be a viable option. This maneuver can potentially provoke bleeding, thereby facilitating clinical observation.[48]
Systemic examination
• General assessment: Conduct a comprehensive check for signs of bleeding (hemorrhage), purpura, or ecchymoses in other parts of the body. Special attention should be paid to the nasal and oral mucosa, as these areas can also provide important clues regarding the source and extent of the bleeding.
• Vital signs: Evaluate key physiological parameters, including blood pressure, blood glucose concentrations, respiratory rate, and pulse rate.
Supplementary investigations based on suspected site of bleeding
• Lacrimal gland origin: When the lacrimal gland is suspected as the origin of bleeding, imaging modalities such as CT and MRI are employed to evaluate the lacrimal gland for the presence of tumors or vascular anomalies. In some cases, a biopsy may be necessary to confirm the diagnosis.
• Conjunctival sac bleeding: For bleeding originating from the conjunctival sac, a cytological analysis of conjunctival scrapings or discharge is performed. This analysis aims to identify the presence of ectopic endometrial cells, neoplastic cells, or foreign substances that may be contributing to the bleeding.[55]
• Punctal bleeding (lacrimal system origin):
○ Lacrimal passage irrigation: This procedure is carried out to assess for stenosis or obstruction of the lacrimal passage and to observe for any bloody reflux, which can indicate a problem within the lacrimal system.
○ Nasal endoscopy: Nasal endoscopy is performed to evaluate the status of the nasal mucosa and to identify any masses that may be present and potentially contributing to the bleeding.
○ Advanced imaging: Advanced imaging techniques, such as Dacryocystography with 3D reconstruction (DCG-CT), orbital or head MRI, or Digital Subtraction Angiography (DSA) may be required to accurately identify masses or vascular leakage within the lacrimal system.
○ Dacryoendoscopy: Dacryoendoscopy is a procedure that allows for direct observation of the lacrimal passages. It enables the identification of intraluminal foreign bodies, mucosal abnormalities, abnormal vascular structures, or neoplasms. This procedure serves both diagnostic and therapeutic purposes.[61, 67]
• Conjunctival foreign body: If a foreign body is identified in the conjunctiva, further inquiry into the patient’s life history is warranted. Additionally, a psychological evaluation should be considered if factitious disorder is suspected.
Laboratory and ancillary tests
• Routine laboratory tests: These include a complete blood count (CBC), a comprehensive metabolic panel, a coagulation profile (comprising prothrombin time (PT), activated partial thromboplastin time (aPTT), international normalized ratio (INR), and fibrinogen levels), and a urinalysis.
• If abnormalities or systemic disease suspected:
○ Coagulation studies: If initial coagulation test suggests a coagulopathy, a full coagulation factor panel should be conducted to further investigate the underlying cause.
○ Vascular imaging techniques: When there is a suspicion of vascular malformations or permeability abnormalities, imaging techniques Digital Subtraction Angiography such as magnetic resonance angiography (MRA), computed tomography angiography (CTA), or digital subtraction angiography (DSA) should be employed. These techniques offer detailed visualization of the vascular system and can help identify any structural or functional abnormalities.
○ Color doppler ultrasound: This imaging modality should be utilized as necessary for targeted vascular evaluations, particularly when assessing blood flow and identifying any vascular occlusions or abnormalities.
○ Capillary fragility test: This test helps diagnose capillary defects or coagulation abnormalities by assessing the fragility of the capillaries under controlled conditions.
○ Allergy workup: In cases where allergic rhinitis is suspected, allergen screening and nasal endoscopy are recommended. Additionally, a diagnostic trial involving anti-allergy medication may be warranted to confirm the diagnosis and assess the effectiveness of treatment.
○ Autoimmune workup: If an autoimmune etiology is suspected, the assessment should include the measurement of C-reactive protein (CRP), pathogen testing, immunological assays, occult blood tests, and abdominal imaging. These tests help identify any underlying autoimmune processes that may be contributing to the patient’s symptoms.
○ Thyroid function assessment: In cases of abnormal thyroid function tests, it is advisable to conduct orbital computed tomography (CT) or magnetic resonance imaging (MRI) to evaluate potential thyroid-related ocular alterations.
○ Gardner-Diamond syndrome test: The diagnostic approach for Gardner-Diamond syndrome may involve the injection of autologous red blood cells or stroma to provoke bruising or bleeding. This provocative test can aid in the diagnosis by reproducing the characteristic symptoms of the syndrome.
○ Endometriosis assessment: The Medroxyprogesterone acetate test is utilized to evaluate cyclical bleeding patterns, serving as a diagnostic tool to exclude the presence of endometriosis, which can sometimes present with atypical bleeding symptoms.
• Multidisciplinary consultation: It is crucial in cases where the presence of bloody tears implicates various bodily systems or requires the expertise of multiple medical specialties. This collaborative approach ensures that all aspects of the patient’s condition are thoroughly evaluated and managed, leading to more accurate diagnoses and effective treatment plans. (This is particularly essential when bloody tears involve multiple systems or specialties.)
Other specialized examinations
• Psychological evaluation: A psychological evaluation is warranted when patients present with a history of abnormal behavior, a diagnosed mental illness, or a life history that may predispose them to excessive mental stress.
• Genetic testing: Genetic testing may be considered in specific clinical scenarios to identify mutations associated with extracellular matrix proteins, collagen, ADAMTS metalloproteinases, mucins, or von Willebrand factor.[87]
Approach to idiopathic cases
When a thorough and comprehensive diagnostic workup fails to pinpoint an organic or psychological cause for the patient’s symptoms, a diagnosis of idiopathic haemolacria may be considered. Nevertheless, it is imperative that such cases undergo long-term follow-up. This follow-up should include periodic re-evaluation of the patient’s condition, and the repetition of relevant investigations if the symptoms either change or persist over time.
Treatment strategies and management
The management of bloody tears is closely tied to the underlying etiology. Since bloody tears can stem from local pathologies with the ocular region, systemic diseases affecting multiple organs, or psychological factors, and may involve multiple systems, a multidisciplinary approach is frequently essential. The treatment process, as illustrated in Figure 1, offers a well-organized and structured framework for selecting the most appropriate therapies.
General principles
Treatment should be precisely customized according to the specific cause that has been pinpointed during the diagnostic evaluation process. In instances where both local and systemic contributing factors are present, or when haemolacria serves as an ocular manifestation of a systemic disease, collaborative management that involves ophthalmologists as well as other specialists (such as hematologists, immunologists, endocrinologists, psychiatrists) is crucial.
Management of local pathologies
Local lesions represent the most prevalent cause of bloody tears. The fundamental treatment principle is the thorough removal or resolution of the pathological lesion, with histopathological examination of the excised tissue being of utmost importance.
• Lacrimal gland tumors: Surgical excision of the tumor is the initial step, followed by pathological diagnosis to determine its nature. Depending on the tumor’s characteristics, adjuvant anti-tumor therapy, such as chemotherapy or radiotherapy, may be necessary. In cases of lacrimal adenitis (inflammation of the lacrimal gland), adjunctive medical therapy might be required to alleviate the inflammation.
• Conjunctival lesions/injuries: The treatment involves excising the pathological tissue and addressing the primary underlying disease, which could be an infection or inflammation.
• Lacrimal drainage system pathologies: These are the most common culprits behind severe bloody tears.
o Canalicular lesions/foreign bodies: Dacryoendoscopic exploration is the preferred method to locate and remove the lesion or foreign body. In some cases, canaliculotomy may be indispensable to gain better access for removal.
o Lacrimal sac/nasolacrimal duct lesions: For benign lesions, dacryocystectomy (excision of the lacrimal sac) is performed to eliminate the lesion, and the excised tissue is then subjected to histopathological examination. The emphasis is on the complete removal of the pathological tissue. Subsequently, reconstruction of the lacrimal passage is essential to restore normal tear drainage function. Surgical options for reconstruction include conjunctivodacryocystorhinostomy (CDCR), conjunctivonasal anastomosis, or canaliculonasal anastomosis. For malignant lesions, a wider is required to restore tear drainage function. For malignant lesions, wider surgical excision is necessary, prioritizing oncological clearance over functional preservation. Secondary lacrimal reconstruction may be considered at a later stage.
• Endometriosis: Cases of ocular or lacrimal endometriosis causing bloody tears require co-management with gynecologists.
Management of systemic conditions
Systemic diseases, which commonly involve the hematologic, immune, or endocrine systems, can be the sole cause of bloody tears or act as confounding factors. They may result in isolated bloody tears haemolacria or bleeding at multiple sites.
• Management primarily entails treating the underlying systemic disease, which often necessitates referral to or consultation with the relevant specialist. Ophthalmologists play a role in follow-up and manage ocular manifestations.
• For bloody tears caused by increased vascular permeability due to abnormal vessels, treatment depends on identifying the location of the abnormal vasculature and may require collaboration with other specialists (e.g., interventional radiologists).
Management of special etiologies
• Drug-induced haemolacria: Diagnostic withdrawal of the suspected offending drug, along with ophthalmological follow-up.
• Vitamin C deficiency-related haemolacria: a trial treatment with vitamin C supplementation can be considered.[59]
• Psychogenic haemolacria: After excluding or treating any identifiable organic causes, patients should be referred for psychiatric diagnosis and treatment. Ophthalmological follow-up should be maintained.[78]
• Idiopathic haemolacria: Requires long-term follow-up. Psychological support and intervention to reduce stress can be beneficial. Lifestyle and environmental modifications may be suggested.
o Pharmacotherapy may be considered cautiously in some cases, including propranolol, metoprolol tartrate, oryzanol, vitamin C, and Yunnan Baiyao capsules. The use of β-blockers like propranolol in children or patients with cardiac conditions must be under the supervision of a cardiologist, and the drug should be discontinued immediately if adverse effects occur.[78,81,89,91,98]
Management of undetermined etiology bloody tears
When extensive investigations fail to pinpoint a clear cause for bloody tears, consideration may be given to treating potential underlying systemic diseases as a form of diagnostic therapy.[86] However, the proactive use of medication in such scenarios remains a matter of debate.
Although most cases of idiopathic haemolacria in adolescents tend to resolve spontaneously by adulthood with few severe consequences, clinicians should not become complacent. The priority is always to actively search for an underlying cause, as some cases of bloody tears may masquerade as idiopathic hemolacria. If no definitive cause is found, close follow-up is essential. If episodes worsen during follow-up, proactive management strategies should be implemented.[58] The treatment flowchart (Figure 1) is designed to assist clinicians in selecting appropriate management strategies based on the diagnosed or suspected cause.
Correction notice
None
Acknowledgements
This consensus was developed by the collective effort
of the following experts and committees.
Sponsoring organizations
Lacrimal Diseases Professional Committee of Ophthalmologist Branch of the Chinese Medical Doctor Association, Lacrimal Disease Group of the Ophthalmic Professional Committee of the Chinese Association of Integrated Medicine
Lead authors (writing experts)
Hai Tao, Fang Bai (Department of Ophthalmology, The Third Medical Center of Chinese PLA General Hospital)
Other expert panel members
Daihui Yang (Second Affiliated Hospital of Nanjing Medical University), Lin Ye (Shenzhen Eye Hospital, Shenzhen Eye Medical Center, Southern Medical University), Zhichong Wang (Zhongshan Ophthalmic Center, Sun Yat-sen University), Mingwu Li (Peking University People's Hospital), Xuanwei Liang (Zhongshan Ophthalmic Center, Sun Yat-sen University)
Other members (alphabetical by pinyin)
Ping Bai (Hebei Eye Hospital), Linlin Chen (Shenyang Fourth People's Hospital), Jianhua Chen (Affiliated Eye Hospital of Shandong University of Traditional Chinese Medicine), Rongxin Chen (Zhongshan Ophthalmic Center, Sun Yat-sen University), Mianzheng Cheng (Wuhan Aige Eye Hospital), Jinlu Fan (Xiamen University Affiliated Eye Center), Jing Gao (Central Hospital of Yingkou Economic and Technological Development Zone, Liaoning), Shuang Geng (Peking Union Medical College Hospital, Chinese Academy of Medical Sciences), Jingwen Gong (Zhejiang Provincial People's Hospital), Sheng Guo (The Fifth People's Hospital of Datong, Shanxi), Shangchen Hao (The First Affiliated Hospital of Zhengzhou University), Youjuan Hao (Yantaishan Hospital, Yantai), Bo Huang (Shenzhen Hospital of Beijing University of Chinese Medicine), Mingli Ji (The Second Affiliated Hospital of Xi'an Medical College, Shanxi), Baoyun Jia (The First Affiliated Hospital of Dali University, Yunnan), Jin Jiang (Zhejiang Provincial People's Hospital), Guangyu Li (The Second Hospital of Jilin University), Xiaodong Li (Guizhou Provincial People's Hospital), Hai Liu (Affiliated Hospital of Yunnan University), Hong Liu (The First Affiliated Hospital of Guangzhou University of Chinese Medicine), Jianju Liu (The First Affiliated Hospital of Harbin Medical University), Mingjiao Liu (Hainan Provincial People's Hospital), Weifeng Liu (Shaoyang Aier Eye Hospital) , Ciren Luobu (Lhasa People's Hospital, Tibet), Hongling Lü (The Second People's Hospital of Foshan, Guangdong), Ya Mo (Affiliated Hospital of Chengdu University of TCM), Gaoxiang Ouyang (Dalian Third People's Hospital Affiliated to Dalian University of Technology), Shuling Pan (Shanghai Aier Eye Hospital), Ronghai Pan (Affiliated Hospital of Xuzhou Medical University, Jiangsu), Zuoxiang Pang (Weifang Eye Hospital, Shandong), Liping Qiao (Armed Police Characteristic Medical Center), Huiling Qing (Henan Provincial People's Hospital), Xiushui Shan (Tangshan Eye Hospital, Hebei), Hongmei Sun (The First Hospital of Tsinghua University), Juhui Tan (Huarong Aier Eye Hospital), Yunhai Tu (Eye Hospital of Wenzhou Medical University), Haibin Wang (Affiliated Hospital of Chengde Medical College), Lihua Wang (The Third Medical Center of Chinese PLA General Hospital), Peng Wang (The Third Medical Center of Chinese PLA General Hospital), Xiuli Wang (Xiamen Eye Center of Xianmen University ), Shijun Wang (Balin Left Banner Traditional Chinese and Mongolian Medicine Hospital, Inner Mongolia), Tingting Wang (Xuzhou First People's Hospital, Jiangsu), Xinming Wang (Beijing Xiren Hospital), Yan Wang (Eye & ENT Hospital of Fudan University),Yao Wang (The Second Affiliated Hospital of Jiamusi University, Heilongjiang), Yuan Wang (Shenzhen Eye Hospital, Shenzhen Eye Medical Center, Southern Medical University), Zhanbin Wu (Shanxi Yuncheng Eye Hospital), Pan Xiao (The Fourth Affiliated Hospital of Soochow University), Shibo Xiong (Wuhan Aige Eye Hospital), Wenshuang Xu (Qiqihar ENT Hospital, Heilongjiang), Chaoyang Xu (Fujian Provincial Hospital Affiliated to Fujian University of TCM), Guangchang Xu (The Second Hospital of Tianjin Medical University), Song Yan (Ordos Central Hospital, Inner Mongolia), Chunfang Yan (Shanxi Eye Hospital), Dikang Yang (Nanchang Purui Eye Hospital), Haijiang Yang (Nanchang Bright Eye Hospital), Hua Yang (Xi'an No.1 Hospital), Jianwei Yang (Hebei Eye Hospital), Jing Yang (Kangba Eye Center, Ganzi Tibetan Autonomous Prefecture People's Hospital, Sichuan), Wen Yang (Shenyang Ninth People's Hospital, Liaoning), Wenhui Yang (Tianjin Medical University General Hospital), Xiaozhao Yang (Xi'an No.1 Hospital), Xueli Yang (Yantaishan Hospital, Shandong), Quan Yin (Ordos Central Hospital, Inner Mongolia), Zhiyun Zhan (The First Affiliated Hospital of Fujian Medical University), Hong Zhang (The First Affiliated Hospital of Xinjiang Medical University), Wenjun Zhang (The 940th Hospital of Joint Service Support Forces of the Chinese PLA), Yi Zhang (Jinzhou Aier Eye Hospital), Zongsheng Zhang (Hami Central Hospital, Xinjiang), Qun Zhang (Nanjing Aier Eye Hospital), Yingjie Zheng (Shanghai University Affiliated Shanghai Heping Ophthalmic Hospital), Sha Zheng (The First Affiliated Hospital of Army Medical University), Yanxia Zheng (CangZhou Hospital of Integrated Traditional Chinese and Western Medicine, Hebei), Jianguang Zhong (Hangzhou First People's Hospital, Zhejiang), Yue Zhong (Yingkou Integrative Medicine Hospital, Liaoning), Dan Zhou (The First Dongguan Affiliated Hospital, Guangdong Medical University), Xibin Zhou (The Third Medical Center of Chinese PLA General Hospital), Hongwei Zhu (The First People's Hospital of Aksu Prefecture, Xinjiang).
Conflict of interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form.
Patient consent for publication
None
Ethical statement
None
Provenance and peer review
This article was a standard submission to our journal. The article has undergone peer review with our anonymous review system.
Data sharing statement
None
Open access statement
This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License(CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited(including links to both the formal publication through the relevant DOI and the license).
Translation note
This article is an English translation of a paper originally published in Yanke Xuebao (眼科学报), Vol. 40, No. 1, pp. 1–11, Year 2025. Original Chinese version DOI: 10.12419/24102302.