Compressive Optic Neuropathy Caused by Cholesterol Granuloma in the Posterior Ethmoid Sinus
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
摘要
Purpose: Cholesterol granuloma is usually associated with chronic middle ear disease.Involvement of the ethmoid sinus by cholesterol granuloma is rare.We describe a case with cholesterol granuloma of the posterior ethmoid sinus causing optic nerve compression. No previous reports were found in our review of the literature.
Case report: A 48-year-old man had impaired visual acuity and a relative afferent pupillary defect in the right eye. Fundus fluorescein angiography showed a swollen optic nerve head and optic disc leakage. Automated perimetry revealed a severe peripheral visual field defect with tunnel vision. Computerized tomography demonstrated an expansile, isodense mass in the right posterior ethmoid sinus, remodeling of the bony walls of the right sphenoid sinus, and lateral displacement of the optic nerve in the right orbit.Compressive optic neuropathy caused by posterior ethmoid sinus lesion was diagnosed.A transnasal endoscopic exploration of the right ethmoid sinuses demonstrated a soft expansile cystic lesion with a thick yellow cap sule that filled the inside of the posterior ethmoid sinus. Brownish fluid with shiny crystals was drained by fine needle aspiration. The capsule was removed completely, and the mucociliary clearance of the sinus was reestablished.The pathologic pictures confimed the diagnosis of cholesterol granuloma, which included typical cholesterol clefts surrounded by inflammatory cells with focal multi-nucleated giant cells.Visual function fully recovered without recurrent lesions after a three-year follow-up.
Conclusion:Compressive optic neuropathy can be rarely caused by cholesterol granuloma in the posterior ethmoid si nus.The visual prognosis may be good after transnasal endoscopic decompression in such patients.
全文
Introduction
Cholesterol granuloma is usually associated with chronic middle ear disease and is relatively rare in the paranasal sinuses¹. The most common location for cholesterol granuloma in paranasal sinuses is the maxillary sinus. l To date, involvements of the ethmoid sinus by cholesterol granuloma have been reported in three cases2-4. To our knowledge, this is the first case of cholesterol granuloma of the posterior ethmoid sinus causing optic nerve compression.
Case report
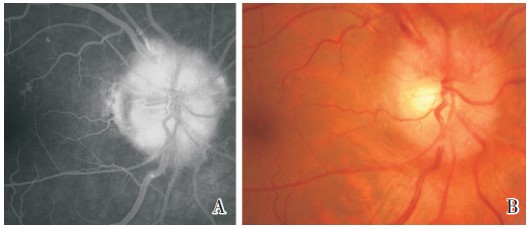
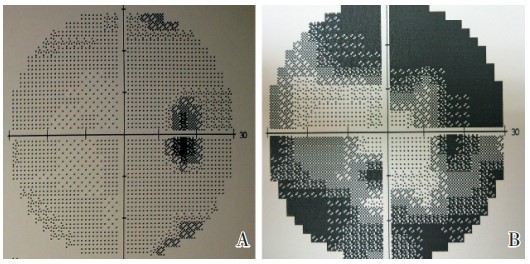
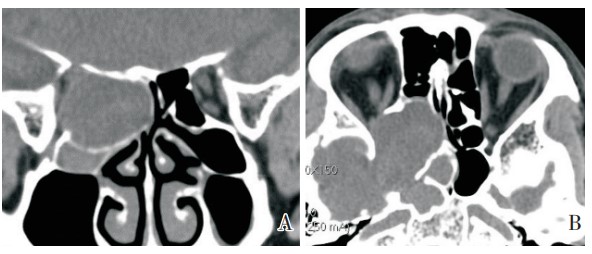
A 48-year-old man complained of progressively blurred vision in the right eye for one month. He had no history of trauma, sinonasal disease, or surgical procedure of the sinuses or eyes. His medical history was unremarkable.His best-corrected visual acuity (BCVA)was 20/25,with a relative afferent pupil lary defect in the right eye. Intraocular pressure,anterior segment,and color vision using Ishihara color plates were normal.Ocular movement was full and free.No proptosis was discovered.Fundus examination showed an apparent swelling of the right optic nerve (Figure lA). Fluorescein angiography showed prominentdiscleakage (Figure lB). Automatedperimetry (Humphrey 30-2 SITA-Standard strategy; Carl Zeiss Meditec, Dublin, CA, USA) revealed a severe peripheral visual field defect with tunnel vision (Figure 2A). Computerized tomography without contrast demonstrated an expansile isodense mass in the right posterior ethmoid sinus (Figures 3A and 3B). Remod eling of the bony walls of the right sphenoid sinus and right maxillary sinus were also noted.The medi al rectus muscle and the optic nerve in the right orbit were laterally displaced.Compressive optic neuropa thy caused by posterior ethmoid sinus lesion was diagnosed.
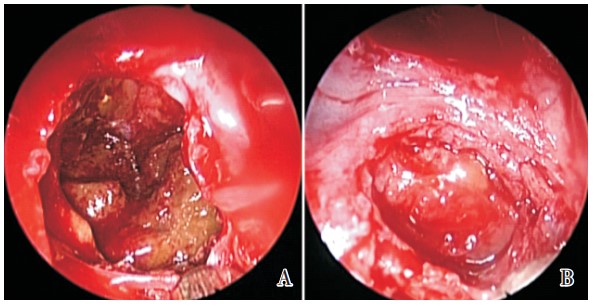
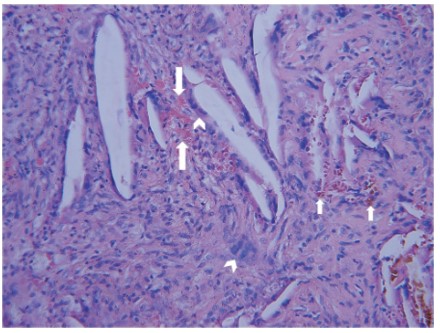
A definite diagnosis and treatment were obtained by performing a transnasal endoscopic exploration of the right ethmoid sinuses.Intra-operatively,the pos terior ethmoid sinus was found to be filled with a soft,expansile,cystic lesion that exhibited a thick yellow capsule(Figure 4A). Fine needle aspiration was performed first and some brownish fluid with shiny crystals was drained. The anterior wall of the capsule was then removed and some yellow-golden, sand-like, semi-fluid substances were noted in the cystic lesion (Figure 4B). The contents, with the anterior, inferior,and medial walls of the capsule, were then removed and the mucociliary clearance of the sinus was reestablished.The pathologic pictures confirmed the diagnosis of cholesterol granuloma, which included typical cholesterol clefts surrounded by inflammatory cells with focal multi-nucleated giant cells and depositions of hemosiderin pigment (Figure 5).
The patient's BCVA improved to 20/20, and a relative afferent pupillary defect disappeared one week after endoscopic sinus surgery. The visual field returned to nearly normal status one month later (Figure 2B). No complications or recurrence had oc curred after three years of follow-up.
Discussion
The hypothetical pathogenesis in cholesterol gran uloma of the paranasal sinus was hemorrhage and obstruction of ventilation⁵.Three cases of cholesterol granuloma involving the ethmoid sinuses were reported in the previous literature2-4. One case with an isolated anterior ethmoid sinus cholesterol granuloma presented with exophthalmos².Another patient with a posterior ethmoid sinus involvement initially com plained of frequent headache.A cholesterol granulo ma was found in the third case in the maxillary and ethmoid sinuses,presenting with sinusitis-like symp toms.All three patients had a history of sinusitis or undergoing surgical procedures over the sinuses,but without any accompanying ocular symptoms and signs. The case in this report is the first case where an ethmoid sinus cholesterol granuloma presented with compressive optic neuropathy without any prior sinonasal disease or procedure.
The proper treatment for paranasal sinus choles terol granuloma is surgical excision¹. An endoscopic approach provides minimized wounds and better cosmetics. However, if cholesterol granuloma occurs in the ethmoid sinus with bony destruction, total excision of the lesion would not be appropriate because of the risk of cerebrospinal fluid leakage or associated orbital complications³. Therefore, as with the treat ment of this case report, endoscopic decompression and removal of the anterior, inferior,and medial walls of the lesion would be adequate in these patients. Careful manipulation of the lateral, posterior, and superior walls is very important to avoid complications.
The overall prognosis of cholesterol granuloma in paranasal sinus is good after operation'.Correct diagnosis and proper excision are important in order to avoid recurrence and complications.Endoscopic de compression of the cholesterol granuloma in this case provided excellent anatomical and functional outcomes without accompanying adverse effects and recurrence.
Only one case of compressive optic neuropathy caused by cholesterol granuloma has been reported previously⁶.That case had sphenoid sinus involvement and a history of sinusitis was noted. Transsphenoidal excision of the cholesterol granuloma eliminated the visual field defect.
Our case reminds us that even in the absence of any history of sinonasal diseases or surgical proce dure of sinuses,cholesterol granuloma is still a dif ferential diagnosis of paranasal sinus lesions.In addition, the insidious progression of this disease located in the ethmoid sinus would lead to compressive optic neuropathy,although it is a rare circumstance.
In conclusion,this case is the first report of posterior ethmoid cholesterol granuloma that presented with progressive visual impairment caused by com pressive optic neuropathy. Pre-operative differential diagnosis for this disease is challenging. However, visual acuity and field could recover soon after en doscopic decompression in these patients.
基金
参考文献
1. Chao TK.Cholesterol granuloma of the maxillary sinus. Eur Arch Otorhinolaryngol,2006,263(6):592-597.
2. Amengot M,Barona R,Garin L,et al.Ethmoid choles- terol granuloma.Otolaryngol Head Neck Surg,1993,109 (4):762-765.
3. Nakagawa T,Asato R,Ito J.Cholesterol granuloma of the posterior ethmoid sinus mimicking meningocele.Acta O- tolaryngol Suppl,2007,557:47-50.
4. Astarci HM,Sungu N,Samin EE,et al.Presence of cholesterol granuloma in the maxillary and ethmoid si- nuses.Oral Maxillofac Surg,2008,12(2):101-103.
5. Friedmann I.Epidermoid cholesteatoma and cholesterol granuloma;experimental and human.Ann Otol Rhinol Laryngol,1959,68(1):57-79.
6. Hwang DJ,Chung YS,Jun SY,et al.A case of compres- sive optic neuropathy caused by sphenoid sinus choles terol granuloma.Jpn J Ophthalmol,2009,53(4):433-434.