


HIGHLIGHTS
1. Critical Discoveries and Outcomes
• Over a decade (2014–2024) and 211,740 phacoemulsification procedures at a high-volume Chinese tertiary day-surgery center, the incidence of postoperative endophthalmitis remained exceptionally low and stable at0.12‰, comparable to the lowest rates reported in Europe, North America, and Japan.
• Multivariable analysis identified male sex, intraoperative complications, and higher Charlson Comorbidity Index score as the main risk factors.
2. Methodological Innovations
• A matched case–control design pairing each case with three controls operated by the same surgeon on the same surgical day minimized confounding from surgeon skill, surgical environment, and temporal factors.
3. Prospective Applications and Future Directions
• The Charlson Comorbidity Index (CCI) offers surgeons a practical, composite preoperative tool to stratify systemic risk, supporting targeted patient education and intensified postoperative monitoring.
• Multivariable analysis identified male sex, intraoperative complications, and higher Charlson Comorbidity Index score as the main risk factors. The center's standardized aseptic protocol and routine intracameral prophylaxis provide a transferable reference model for Chinese hospitals expanding day-surgery programs.
Introduction
Cataract surgery is one of the most performed ophthalmic procedures globally.[1] As a developing country with a population of 1.4 billion Chinese has seen its cataract surgical rate (CSR) doubled over the decades (2010-2015), and it is estimated to reach 4,287 cases per million people by 2025.[2] Efficient implementation of cataract surgery requires paramount attention to the management of postoperative complications. Among these, postoperative endophthalmitis (POE) remains a rare but vision-threatening challenge for most cataract surgeons.
The incidence of endophthalmitis in China ranges from 0.03%-0.1% across different regions and institutions, according to a 2013 multi-center study.[3] While previous studies have identified risk factors such as intraoperative complications and prolonged operation time,[4] their findings are inconsistent and often limited by data quality and varying infection control standards. To date, few longitudinal studies have analyzed the long-term trends in POE in incidence, and existing reports are frequently constrained by small sample sizes or the absence of matched controls. Understanding trends in endophthalmitis incidence is crucial for developing nations such as China, which has experienced a rapid expansion of high-volume cataract surgery, accompanied by increasing adoption of outpatient (day-surgery) models and shortened hospital stays.[5-6] With over a decade of experience and a daily volume exceeding 100 procedures, Zhongshan Ophthalmic Center (ZOC) , Sun Yat-sen University is one of the pioneers of cataract day surgery in China.[7] Given its high volume and standardized perioperative protocols, the center's endophthalmitis incidence and risk factor profile may offer a valuable reference for other Chinese hospitals planning to establish day surgery programs.
Therefore, we conducted a 10-year retrospective matched case–control study in this high-volume Chinese ophthalmic centre. The purpose of our study was to: (1) report the annual trends of POE after phacoemulsification, and (2) investigate major clinical risk factors, and (3) describe microbiological findings within this period of evolving infection control policies.
Methods
Study design and setting
A retrospective matched case–control study was conducted at ZOC, Guangzhou, China. All consecutive cataract surgeries performed between January 2014 and December 2024 were identified via electronic medical records. Individual informed consent was waived due to the anonymized retrospective design. Case groups were defined as patients who underwent cataract extraction surgery at ZOC and were diagnosed with acute postoperative endophthalmitis within 6 weeks of surgery. Diagnosis was confirmed by experienced ophthalmologists and recorded by the infection surveillance department. Among 211,740 eyes undergoing cataract surgery, 25 were identified as cases (POE group). For each case, 3 controls were randomly selected from the same surgeon’s patient list on the same surgical day who did not develop endophthalmitis, resulting in a 1:3 case-to-control ratio. This matching strategy was adopted to minimize the impact of confounding factors such as surgeon skill, surgical environment, and temporal factors.
Data collection
In accordance with the standardized infection-control protocol at ZOC, all patients undergoing cataract surgery received a uniform perioperative antimicrobial regimen. Preoperatively, broad-spectrum topical antibiotics (levofloxacin or gatifloxacin eye drops) were routinely administered for 3 days before surgery. On the day of surgery, the conjunctival sac was thoroughly irrigated and cleaned, followed by sterile draping. Immediately before incision, a 5% povidone-iodine solution was applied to the ocular surface and conjunctival sac. At the end of surgery, all patients received an intracameral antibiotic injection of either cefuroxime or vancomycin. This prophylactic strategy evolved in 2015: vancomycin was used exclusively before 2015, whereas cefuroxime was subsequently adopted as the first-line agent, with vancomycin reserved for complex or high-risk cases in accordance with institutional infection-control recommendations.
Preoperative and intraoperative characteristics of cases and controls were compared. Demographic, systemic, and ocular biometric data were extracted from the electronic medical records. Demographic data including information on sex, age, region, education status, eye laterality, history of ocular disease and intraocular surgery, systemic comorbidities, and Charlson Comorbidity Index (CCI) score. Prior intraocular surgery included previous pars plana vitrectomy, scleral buckling or encircling procedures, and silicone oil injection or removal. The age-adjusted CCI was used to quantify overall comorbidity burden, incorporating both the weighted scores of 19 comorbidity categories and an age component (one point added per decade above 40 years), with higher scores indicating greater systemic disease burden. Perioperative details such as surgical technique, intraocular lens (IOL) type, operation time, combined procedures, intraoperative complications and the agent used for intracameral antibiotic prophylaxis were also collected.
Statistical analysis
Continuous variables were summarized as mean ± SD and compared using the t test or Mann–Whitney U test. Categorical variables were expressed as frequencies (%) and compared by χ2 or Fisher’s exact test. Annual incidence rates were calculated as the number of POE cases per 10,000 cataract surgeries with 95 % Poisson confidence intervals. Trends over time were assessed using Poisson regression with surgical year as a continuous variable, the Cochran–Armitage trend test was also conducted as sensitivity analysis.[8]
Univariate and multivariate logistic regression analyses were performed to identify independent risk factors. Given the small sample size, variables with P < 0.10 in univariate analysis or of clinical interest (sex, prior surgery, combined procedure, CCI) were included in the final model. Conditional and exact logistic regressions were further conducted as sensitivity analyses stratified by surgeon × surgery-date. Odds ratios (OR) and 95 % confidence intervals (CI) were reported. Analyses were performed using Stata 17.0 (StataCorp, College Station, TX, USA) and R (Foundation for Statistical Computing). A two-sided P< 0.05 was considered statistically significant.
Results
Incidence and temporal trend
Between 2014 and 2024, approximately 211,740 phacoemulsification procedures were performed at Zhongshan Ophthalmic Center, Sun Yat-sen University. 25 patients were diagnosed with postoperative endophthalmitis, yielding an overall incidence of 0.12‰. Annual rates remained remarkably low throughout the decade with no sustained increase after 2015 (Figure 1). The annual incidence of postoperative endophthalmitis ranged from 0.02 to 0.05‰. Poisson regression demonstrated a mild upward trend over time (β = 0.145, P = 0.024). The Cochran–Armitage trend test confirmed this finding (χ2 = 5.6, P = 0.02). Although statistically significant, the absolute incidence remained extremely low throughout the decade. Sensitivity analyses were also stratified by year 2015 (change for intracameral antibiotic injection) and 2019 (the pre-/post-COVID period), no significant change in incidence trends was detected across either cut-off (interaction P = 0.41 for 2015, P = 0.27 for 2019).
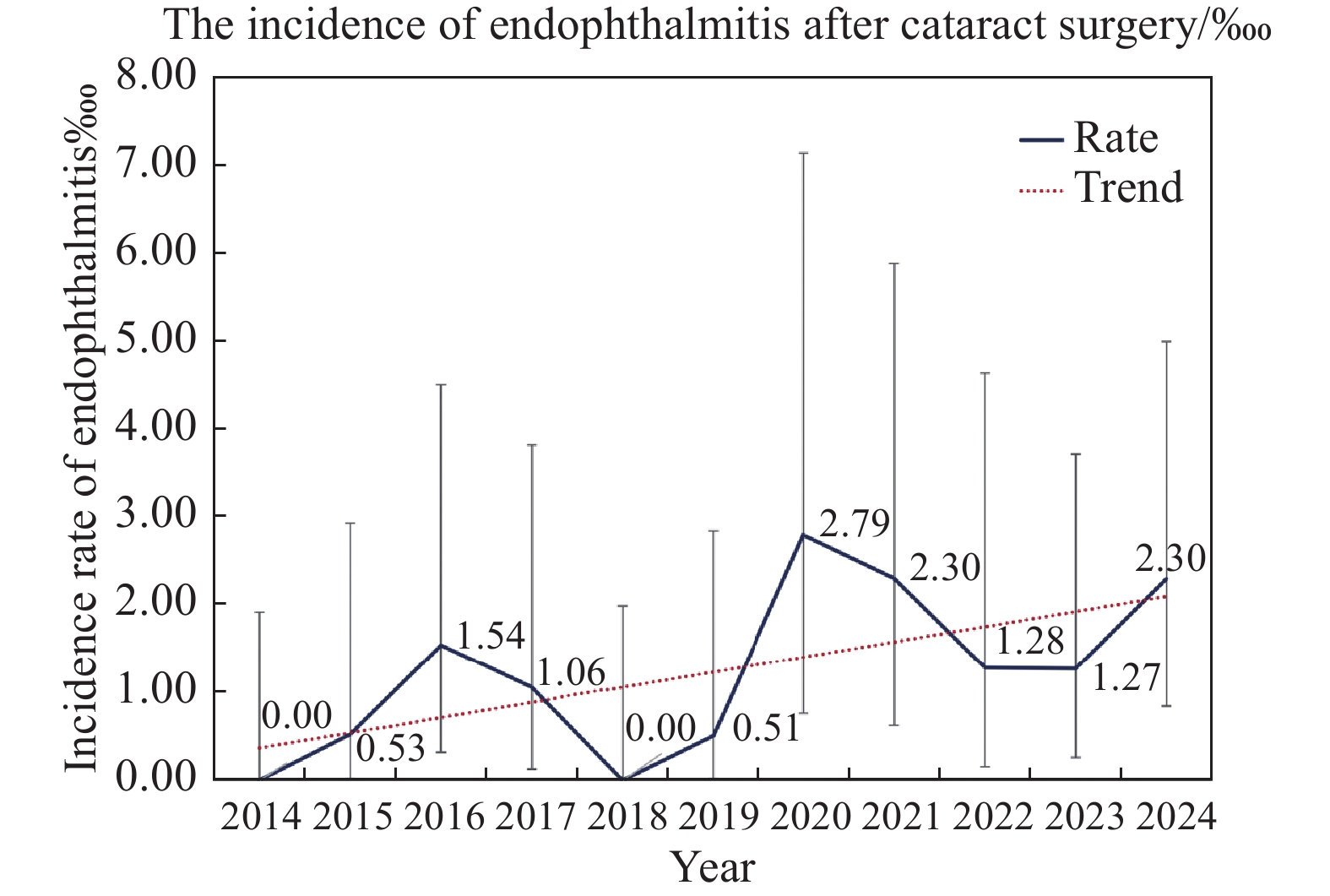
Blue line represents the annual incidence of postoperative endophthalmitis, expressed per 1,000 cataract surgeries. The red dotted line denotes the fitted temporal trend based on Poisson regression. Error bars indicate 95% Poisson confidence intervals.
Baseline characteristics
The demographic and clinical characteristics of 25 cases and 75 matched controls are listed in Table 1. The POE group exhibited a significantly greater proportion of males (28% vs. 68%, P < 0.001) and higher rates of both intraoperative complications and concurrent surgical procedures, such as anterior vitrectomy or pupiloplasty (complication rate: 16% vs. 1.33%, P = 0.018). A history of prior intraocular surgery was also more common among POE group (20% vs. 5.33%, P = 0.027). Additionally, the mean CCI score was significantly elevated in the POE group (0.72 ± 1.11 vs. 0.23 ± 0.51, P = 0.032). No other significant difference in baseline demographic or postoperative characteristics was observed between the groups, including eye laterality, diabetes and hypertension status, residential area, or visual acuity and IOP at postoperative day 1.
|
|
POE Group (n=25) |
Control Group (n=75) |
P value |
|
Baseline characteristics |
|
|
|
|
Age at time of surgery, mean ± SD, years |
59.10 ± 18.26 |
62.89 ± 18.14 |
0.13 |
|
Gender, female, n(%) |
7(28) |
51(68) |
<0.001 |
|
History of intraocular surgery in operative eye, n(%) |
5(20) |
4(5) |
0.03 |
|
Eye laterality, n(%) |
|
|
0.49 |
|
Right |
11(44) |
39(52) |
|
|
Left |
14(56) |
36(48) |
|
|
Region |
|
|
0.71 |
|
City |
18(72) |
51(68) |
|
|
Country |
7(28) |
24(32) |
|
|
Educational Status |
|
|
0.55 |
|
Elementary school graduate or less |
6(24) |
22(29) |
|
|
Middle school graduate |
3(12) |
10(13) |
|
|
High school graduate |
4(16) |
17(23) |
|
|
College graduate or higher |
5(20) |
6(8) |
|
|
N/A |
7(28) |
20(27) |
|
|
Hypertension, n(%) |
7 (28) |
28 (37) |
0.40 |
|
Diabetes, n (%) |
3 (12) |
12 (16) |
0.68 |
|
Charlson Comorbidity Index score |
0.72 ± 1.11 |
0.23 ± 0.51 |
0.01 |
|
Perioperative characteristics |
|
|
|
|
Duration of surgery, mean ± SD, minutes |
15.80 ± 10.60 |
13.05 ± 10.52 |
0.37 |
|
Cataract Surgery Concurrent with another ophthalmic procedure, n(%) |
4 (16) |
3 (4) |
0.04 |
|
Intraoperative Comlications Requiring Anterior Vitrectomy, n(%) |
4 (16) |
1 (1) |
0.01 |
|
Visual Acuity at 1d after surgery logMAR, mean ± SD* |
0.40 ± 0.43 |
0.55 ± 0.43 |
0.18 |
|
IOP at 1d after surgery, mean ± SD, mmHg |
14.36 ± 5.20 (range: 7-33) |
14.38 ± 5.18 (range: 7-30) |
0.83 |
Risk factor analysis
Results of risk factor analysis were presented in Table 2. Univariate logistic analysis revealed that male sex (OR=3.46, 95%CI 1.45-8.26), prior intraocular surgery (OR=4.44, 95%CI 1.09-18.09), combined intraocular procedures (OR=5.8, 95%CI 1.3-25.96), intraoperative complications (OR=22.26, 95%CI 1.49-132.97), and higher CCI scores (OR=2.39, 95%CI 1.18-4.85) were independent risk factors for POE (all P < 0.05). Multivariable logistic regression further confirmed three independent predictors of POE: male sex (OR=2.60, 95%CI 1.01–6.68), intraoperative complications (OR=18.32, 95% CI 1.94–172.75), and higher Charlson CCI score (OR=1.625 per point, 95%CI 1.01–2.62). The reliability of these factors was further verified by sensitivity analyses using conditional and exact logistic regression, which yielded comparable estimates.
|
|
Univariate Logistic Analysis Odds Ratio (95% CI) |
Multivariate Logistic Analysis Odds Ratio (95% CI) |
|
Sex |
|
|
|
Male |
3.46(1.45, 8.26) |
2.60 (1.01, 6.68) |
|
Female |
Reference |
Reference |
|
Age |
0.99 (0.97, 1.01) |
|
|
Region |
|
|
|
City |
Reference |
|
|
Country |
1.23 (0.51, 2.99) |
|
|
Systematic Disease |
|
|
|
Yes |
1.20 (0.46, 3.13) |
|
|
No |
Reference |
|
|
History of intraocular surgery in operative eye |
|
|
|
Yes |
4.45 (1.09, 18.09) |
2.53 (0.55, 11.69) |
|
No |
Reference |
Reference |
|
Concurrent with another ophthalmic procedure |
|
|
|
Yes |
5.8 (1.30, 25.96) a |
|
|
No |
Reference |
|
|
Intraoperative Comlications |
|
|
|
Yes |
22.26 (1.49,132.97) |
18.32 (1.94, 172.75) |
|
No |
Reference |
Reference |
|
Charlson comorbidity score |
2.39 (1.18, 4.85) |
1.625 (1.01, 2.62) |
|
a. Given the potential collinearity between concurrent procedures and intraoperative complications, only the latter was included in the multivariate analysis. |
||
Microbiological findings
The microbiological findings are presented in Table 3. Pathogen detection and culture were performed on 19 specimens, with a culture positivity rate of 31.6% (6/19). The most frequently identified organisms were Pseudomonas aeruginosa (two cases), followed by Candida tropicalis, Enterococcus faecalis, Escherichia coli and a suspected Gram-positive coccus. The median onset interval was 10 days (range, 1-28). Clinically, most patients (68%) underwent aqueous/vitreous biopsy and were treated with intracameral injection (mainly vancomycin), whereas 7 patients required pars plana vitrectomy surgery, including one with IOL explanation. Visual outcomes varied. Among the 25 cases, 5 (20%) achieved a final BCVA of ≤0.3 logMAR, 12 (48%) had a BCVA of 0.3–1.3 logMAR, and 7 (28%) had a BCVA of >1.3 logMAR. The latter group met the criteria for blindness by Chinese national standards. One case (4%) resulted in evisceration due to uncontrolled recurrent infections and secondary glaucoma.
|
|
Cases, n (%) |
Year of diagnosis |
Interval between surgery and endophthalmitis presentation, days |
Treatment |
BCVA at last follow up (logMAR) |
|
Negative culture |
13 (68.42) |
|
|
|
|
|
Positive culture |
6 (31.58) |
|
10.67 |
|
|
|
Pseudomonas aeruginosa |
2 |
2024, 2022 |
2, 23 |
Pars Plana Vitrectomy/ Extraction of intraocular lens |
0.2, 0.6 |
|
Candida tropicalis |
1 |
2024 |
28 |
Pars Plana Vitrectomy/ Extraction of intraocular lens |
0.7 |
|
Streptococcus vestibularis |
1 |
2023 |
4 |
Pars Plana Vitrectomy |
Light following |
|
Enterococcus faecalis |
1 |
2021 |
4 |
Intracameral flushing +injection |
FC/30cm |
|
Escherichia coli/Enterococcus faecalis |
1 |
2017 |
1 |
Pars Plana Vitrectomy |
1.0 |
|
Suspected Gram-positive cocci* |
1(5.26) |
2016 |
4 |
Intracameral flushing +injection |
1.0 |
|
Total |
19 |
|
|
|
|
|
* No bacterial growth was observed in the culture. |
|||||
Discussion
This decade-long analysis at Zhongshan Ophthalmic Center demonstrated that an exceptionally low and stable incidence of post-cataract endophthalmitis (0.12‰) is attainable within a rapidly expanding Chinese day-surgery system. The overall rate was comparable to the lowest figures reported from Europe (0.04‰–0.7‰), North America (0.1‰–1.36‰)[9–11] and Japan, and similar to those reported from Britain.[12-13] Although a mild upward temporal trend was observed, the absolute change was negligible given the very low baseline rate. Segmented Poisson models around 2015 (intracameral policy change) and 2019 (pre/post-COVID period) also showed no significant slope change, supporting the overall temporal stability of POE under standardized infection-control protocols. These observations are consistent with prior evidence indicating that standardized aseptic techniques and routine intracameral antibiotic use are associated with sustained low rates of postoperative endophthalmitis.[14-15]
Multivariable analyses identified male sex, intraoperative complications (e.g., anterior vitrectomy), and a higher CCI score as independent risk factors. Male sex as a risk factor has been consistently reported in large registry-based studies from Asia and Western countries.[16-17] While the underlying mechanisms remain uncertain, differences in ocular surface flora and postoperative care behaviors have been hypothesized. The significance of the CCI as independent risk factor is supported by large registry data showing that overall comorbidity burden, rather than individual conditions alone, better captures susceptibility to postoperative infection.[11,18] In large Medicare analyses, higher Charlson Comorbidity Index scores were associated with an increased risk of postoperative endophthalmitis after cataract surgery, even after adjustment for age, sex, and other factors.[19] Using a composite index such as CCI mitigates collinearity among individual diagnoses and may reflect the impact of systemic frailty and immunologic reserve on postoperative ocular defense.[20] It could also serve as a practical tool for surgeons to evaluate patient risk before surgery.
Culture positivity in our series was about 31.6 %, comparable to within the 30–50% range commonly reported for acute post-cataract POE.[6,21] This low positivity rate likely reflects sterilization by prior antibiotic therapy. Additionally, biofilm formation on the IOL and fastidious organisms such as Cutibacterium acnes often evade standard detection.[22-23] Coagulase-negative Staphylococci (CoNs) remained the predominant isolates.[24] We also identified enteric pathogens, including Enterococcus faecalis and Gram-negative rods (e.g., E. coli). These organisms have garnered increasing attention due to their virulent nature, often leading to poor visual outcomes, and their potential for multidrug resistance. Reviews confirm that Gram-negative infections after cataract surgery are uncommon but clinically important when present, whereas E. faecalis can be highly destructive and may carry resistance determinants.[25] Moreover, we did not observe a shift toward Gram-negative or fungal infections after the 2015 change from intracameral vancomycin to cefuroxime, consistent with national/registry-level evidence that intracameral prophylaxis per se, rather than a specific drug, underpins low POE rates.[26] Based on microbiological findings, we recommend reinforcing basic hygiene education following same-day surgery: strictly adherence to hand cleansing after toilet use, avoidance of eye rubbing, and limited contact with water sources/contaminants (e.g., swimming pools, non-sterile dressings) during the early postoperative period.
Strengths of this study include a 10-year observation window at a high-volume tertiary eye center, matched case–control design (surgeon × surgical date) to limit performance/time-cluster confounding, and sensitivity analyses yielding concordant results. However, the retrospective single-center design and small number of events limited statistical power and widened confidence intervals. Although cases and controls were matched by surgeon and surgical date to control for operative and perioperative confounders, formal propensity score matching could not be performed, as individual-level data for the full surgical cohort were not retrievable for the entire study period. Patient-level baseline imbalance therefore remains a limitation. Future multicenter studies with larger sample sizes would be better positioned to apply PSM and further disentangle surgical and patient-level risk factors for post-cataract endophthalmitis.
In conclusion, an exceptionally low annual POE incidence was maintained in a high-volume Chinese day-surgery ophthalmic center. For male patients and those with higher CCI scores or intraoperative complications, enhanced patient education and intensified postoperative monitoring are warranted. These findings support ongoing adherence to rigorous aseptic techniques and routine intracameral prophylaxis as cornerstones of safe cataract surgery.
Correction notice
None
Acknowledgements
None
Author Contributions
(I) Conception and design: Xiaohang Xie, Haowen Lin, Jiaqing Zhang, Lixia Luo
(II) Administrative support: Jiaqing Zhang, Xuhua Tan, Lixia Luo
(III) Provision of study materials or patients: Jiaqing Zhang, Lixia Luo
(IV) Collection and assembly of data: Xiaohang Xie, Haowen Lin, Xiaozhang Qiu
(V) Data analysis and interpretation: Xiaohang Xie, Haowen Lin
(VI) Manuscript writing: All authors
(VII) Final approval of manuscript: All authors
Conflict of Interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form.
Patient consent for publication
None
Ethics approval and consent to participate
This study was approved by the ZOC review board (2019KYPJ033).
Data availability statement
None
Open access
This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License(CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited(including links to both the formal publication through the relevant DOI and the license).