


HIGHLIGHTS
1. Critical Discoveries and Outcomes
• Cataract surgery significantly improved visual acuity in most cataract patients with congenital iridochoroidal coloboma. Poor preoperative corrected distance visual acuity (CDVA) and the presence of microcornea were identified as significant predictors of poor visual prognosis.
2. Methodological Innovations
• This study identified visual prognostic indicators that do not rely on preoperative fundus examination, which is often limited in patients with dense cataracts. By analyzing routinely accessible clinical parameters and using logistic regression, the study provided a practical non-fundus-based approach for preoperative prognostic assessment in patients with congenital iridochoroidal coloboma.
3. Prospective Applications and Future Directions
• These findings may help ophthalmologists improve surgical decision-making and provide more accurate preoperative counseling for patients with congenital iridochoroidal coloboma. Future larger-scale and long-term studies are needed to validate these predictors and further clarify the mechanisms linking microcornea to poor visual outcomes.
Introduction
Congenital iridochoroidal coloboma is caused by the abnormal closure of the embryonal fissure during development,[1-3] with a prevalence ranging from approximately 0.048% to 0.07%.[4-5] Typically, it manifests as a structural defect involving the iris, choroid, outer retinal layer, and retinal pigment epithelium within the affected area.[4,6] Patients with congenital iridochoroidal coloboma exhibit considerable variability in terms of age of onset, severity, progression, and associated complications, including microphthalmia, microcornea, optic atrophy, strabismus, and nystagmus. Additionally, complications such as cataract, lens subluxation, secondary glaucoma, retinal detachment, amblyopia, anisometropia, and sensory strabismus are frequently reported, with cataract being the most common complication.[4]
Cataract surgery in eyes with iridochoroidal coloboma presents significant challenges due to anatomical anomalies such as inadequate pupil dilation, eccentric pupil position, zonular weakness, small corneal diameter, and restricted space for manipulation within the anterior chamber.[3,7] These factors increase the risk of intraoperative complications, including posterior capsular rupture (PCR), zonular dialysis (ZD), and vitreous prolapse during cataract surgery, particularly in the eyes with hard cataracts.[7] Importantly, previous studies have reported that over 20% of patients with congenital iridochoroidal coloboma have corrected distance visual acuity (CDVA) worse than 20/200 following cataract surgery.[7-8] Given the increased risk of complications, it is essential to carefully weigh the potential benefits of surgery against its risks. Consequently, preoperative evaluation of visual prognosis plays a critical role in determining surgical suitability. It not only guides clinical decision-making but also helps manage patient expectations and improves physician–patient communication.
Assessment of visual prognosis following cataract surgery in patients with congenital iridochoroidal coloboma predominantly depends on the extent of fundus involvement.[8-9] However, due to opacities of refractive media, more than half of patients are unable to undergo detailed fundus examination before cataract surgery.[8] Although visual electrophysiology test (e.g., ERG, VEP) can also be used to assess fundus function, their accuracy may be compromised in the presence of dense cataracts.[10] Therefore, the aim of this study was to identify the visual prognostic indicators independent of fundus examination in congenital iridochoroidal coloboma with cataract. These findings may provide practical insights into surgical decision-making and help optimize the timing of cataract intervention in these patients.
Methods
Data collection
This retrospective study enrolled patients with congenital iridochoroidal coloboma who underwent cataract surgery at Zhongshan Ophthalmic Center, Sun Yat-sen University from January 2022 to October 2024. The study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Zhongshan Ophthalmic Center, Sun Yat-sen University. Due to the retrospective nature of the study, the requirement for informed consent was waived.
Patients were included according to the following criteria: (1) a clinical diagnosis of congenital iridochoroidal coloboma; (2) a history of cataract surgery; and (3) availability of preoperative and postoperative visual acuity data. Exclusion criteria were as follows: (1) a history of severe corneal disease, uveitis, glaucoma, or retinal detachment; (2) cataract surgery combined with retinal surgery; and (3) a follow-up of less than 1 month.
Preoperative clinical data were extracted from electronic medical records, including demographics, medical history, slit-lamp and fundus examination findings, CDVA, intraocular pressure (IOP), axial length (AL), and the presence of strabismus and nystagmus. Cataract density was evaluated using the Lens Opacity Classification System III, with hard nuclear cataract defined as a nuclear opalescence (NO) grade of 5 to 6.[11] In eyes with significant refractive media opacity, B-scan ultrasound was utilized to confirm choroidal coloboma when fundus visualization was uncertain. AL was measured using the Zeiss IOLMaster 700 (Carl Zeiss Meditec AG) or immersion A-scan (Alcon Ultrascan; Alcon Laboratories Inc., Fort Worth, U.S.A). Microcornea was defined as a white-to-white corneal diameter < 10 mm, measured with a focused slit-lamp light beam while the patient was seated. The extent of iris coloboma was quantified by the number of clock hours involved. Intraoperative data were recorded, including details of the surgical procedure, use of a capsular tension ring, and any intraoperative complications (e.g. PCR, vitreous prolapse, dropped nucleus). Postoperative data included CDVA and postoperative complications.
The primary outcome was CDVA at 1 month postoperatively. Secondary outcomes included CDVA at the final visit and the incidence of intraoperative and postoperative complications.
Surgical technique
All surgical procedures were performed by a single experienced surgeon (S.H.). The method of cataract extraction, phacoemulsification (PE) or manual small-incision cataract surgery (MSICS), was determined based on cataract density and associated factors, such as zonular stability. Eyes undergoing PE were planned for IOL implantation, whereas those undergoing MSICS were left aphakic. The decision to implant a capsular tension ring (CTR) was based on the extent of zonular weakness and capsular bag stability.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics software (v. 26.0, IBM Corp.). Preoperative CDVA was classified into categories of visual impairment based on World Health Organization guidelines: no visual impairment (CDVA ≥ 20/40), mild visual impairment (20/67 ≤ CDVA < 20/40), low vision (20/200 ≤ CDVA < 20/67), severe visual impairment (20/400 ≤ CDVA < 20/200) or blindness (CDVA < 20/400).[12-13] For analysis, CDVA was converted to logarithm of the minimum angle of resolution (logMAR) values. The vision classifications of counting fingers, hand motion, light perception, and no light perception were given the logMAR values 2.1, 2.4, 2.7 and 3.0, respectively.[12-13] Comparisons between categorical and continuous variables were conducted using the chi-square test, t-test or Wilcoxon test. Logistic regression models were used to assess the associations between risk factors and poor visual outcomes. Due to the symmetry of both eyes from the individuals, data from the first operated eyes were used for logistic regression analysis. P values less than 0.05 were considered statistically significant.
Results
Patient characteristics
The clinical characteristics of patients are summarized in Table 1. A total of 42 eyes from 36 patients (18 males and 18 females) were included in the study. Among these, 11 eyes had iris-isolated coloboma, and 31 eyes had iridochoroidal coloboma. All patients exhibited typical full-thickness iris coloboma in the inferior quadrant. The mean age at the time of surgery was (45.4 ± 8.2) years (range: 20 to 68 years), and the mean follow-up time was (7.2 ± 3.8) months (range: 1 to 20 months). Bilateral cataract surgery was performed in 6 patients. The mean preoperative CDVA and IOP were (1.50 ± 0.35) logMAR and 16.3 ± 2.2 mmHg, respectively. The mean preoperative AL and ECD were (24.79 ± 2.08) mm and (3,116 ± 395) cell/mm2, respectively.
|
Characteristic |
Total |
|
Patients |
36 |
|
Eyes |
42 |
|
Follow-up time (months) |
7.2±3.8 |
|
Age (y) |
45.4±8.2 |
|
Gender (Male/Female) |
21/21 |
|
Preoperative CDVA (logMAR) |
1.50±0.35 |
|
IOP (mmHg) |
16.3±2.2 |
|
AL (mm) |
24.79±2.08 |
|
ECD (cell/mm2) |
3,116±395 |
|
Hard nuclear cataract (eyes,%) |
20 (47.6%) |
|
Microcornea (eyes,%) |
10 (23.8%) |
|
Strabismus (eyes,%) |
7 (16.7%) |
|
Nystagmus (eyes,%) |
8 (19.0%) |
|
CDVA: corrected distance visual acuity; IOP: intraocular pressure; AL: axial length; ECD: corneal endothelial cell density. |
|
Microcornea was observed in 10 eyes (23.8%). Strabismus and nystagmus were observed in 7 eyes (16.7%) and 8 eyes (19.0%), respectively. Cataract morphology analysis revealed that nucleus sclerosis was the most common type, followed by cortical opacity. A total of 20 eyes (47.6%) were classified as hard nuclear cataracts.
Preoperatively, the fundus was clearly visualized through detailed indirect ophthalmoscopy in only 18 eyes (42.8%). In eyes with dense cataracts, B-scan ultrasonography was used as an alternative. Postoperatively, indirect ophthalmoscopy was performed in all patients to assess the extent of coloboma. Of these, 11 eyes (26.1%) had coloboma involving the disc/macula.
Intraoperative assessment
Phacoemulsification (PE) was performed in 37 eyes (88.1%) and manual small incision cataract surgery (MSICS) in 5 eyes (11.9%), according to cataract density. Uneventful surgery was achieved in 36 eyes (85.7%), while intraoperative complications were recorded in 8 eyes (19.0%). Detailed information on eyes with intraoperative complications is presented in Table 2. In PE group, ZD was observed in 4 eyes, and PCR in 1 eye. Intraocular lens (IOL) were implanted in 36 eyes; one eye did not receive IOL implantation due to PCR. In MSICS group, ZD was noted in 2 eyes and PCR in 1 eye. All eyes in the MSICS group were left aphakic.
|
Age/gender |
Type and grade of cataract |
Complications |
Managements |
Postoperative CDVA |
|
51/M |
N6 |
PCR+nuclear drop |
PE+PPV |
LP |
|
42/M |
N6 |
ZD |
MSICS |
20/400 |
|
38/M |
N6 |
PCR |
MSICS+AV |
FC |
|
39/M |
N6 |
ZD+Vitreous loss |
MSICS+AV |
20/400 |
|
21/M |
N2, ACC |
ZD |
PE+IOL+CTR |
20/40 |
|
68/M |
N3 |
ZD |
PE+IOL+CTR |
20/80 |
|
50/F |
N5 |
ZD |
PE+IOL+CTR |
FC |
|
38/M |
N5 |
ZD |
PE+IOL+CTR |
20/400 |
|
N: nuclear grade; ACC: anterior cortical cataract; PCR: posterior capsule rupture; ZD: zonular dialysis; AV: anterior vitrectomy; PPV: pars plana vitrectomy; PE: phacoemulsification; MSICS: manual small incision cataract surgery; IOL: intraocular lens: CTR: capsular tension ring; FC: counting fingers; LP: light perception. |
||||
Postoperative assessment
Corneal edema was observed in 17 eyes on the first postoperative day and resolved with conservative therapy alone in all cases. Transient IOP elevation occurred in 9 eyes and was managed with IOP-lowering medication. Mild IOL dislocation, not requiring additional surgical intervention, was noted in 2 eyes at 3 and 12 months postoperatively, respectively. One eye developed retinal detachment and underwent pars plana vitrectomy at 6 months postoperatively. None of the patients developed postoperative endophthalmitis.
Figure 1 shows a comparison between preoperative and postoperative CDVA following cataract surgery. The mean CDVA improved from (1.50 ± 0.35) logMAR preoperatively to (0.80 ± 0.52) logMAR at 1 month postoperatively (P < 0.001) and (0.79 ± 0.53) logMAR at the final visit (P < 0.001). Visual improvement, defined as a postoperative CDVA gain ≥ 0.1 logMAR, was observed in 29 eyes (69.0%). Poor postoperative visual prognosis, defined as postoperative CDVA < 1.0 logMAR, was observed in 13 eyes (31.0%). Despite this, eyes with low postoperative CDVA still experienced significant improvement compared with preoperative CDVA (1.51 ± 0.59 vs. 1.86 ± 0.62, P=0.002). Risk factor analysis for poor postoperative visual prognosis is presented in Table 3. Multivariate logistic regression revealed that poor preoperative CDVA (OR= 16.01, 95% CI: 1.38 to 185.40, P = 0.026) and microcornea (OR = 18.65, 95% CI: 1.45 to 240.52, P = 0.025) were associated with poor postoperative visual outcomes. Among these eyes, coloboma involving with disc/macula was detected in 10 eyes (23.8%). Figure 2 shows representative cases of two patients with similar dense cataract but distinct visual prognosis.
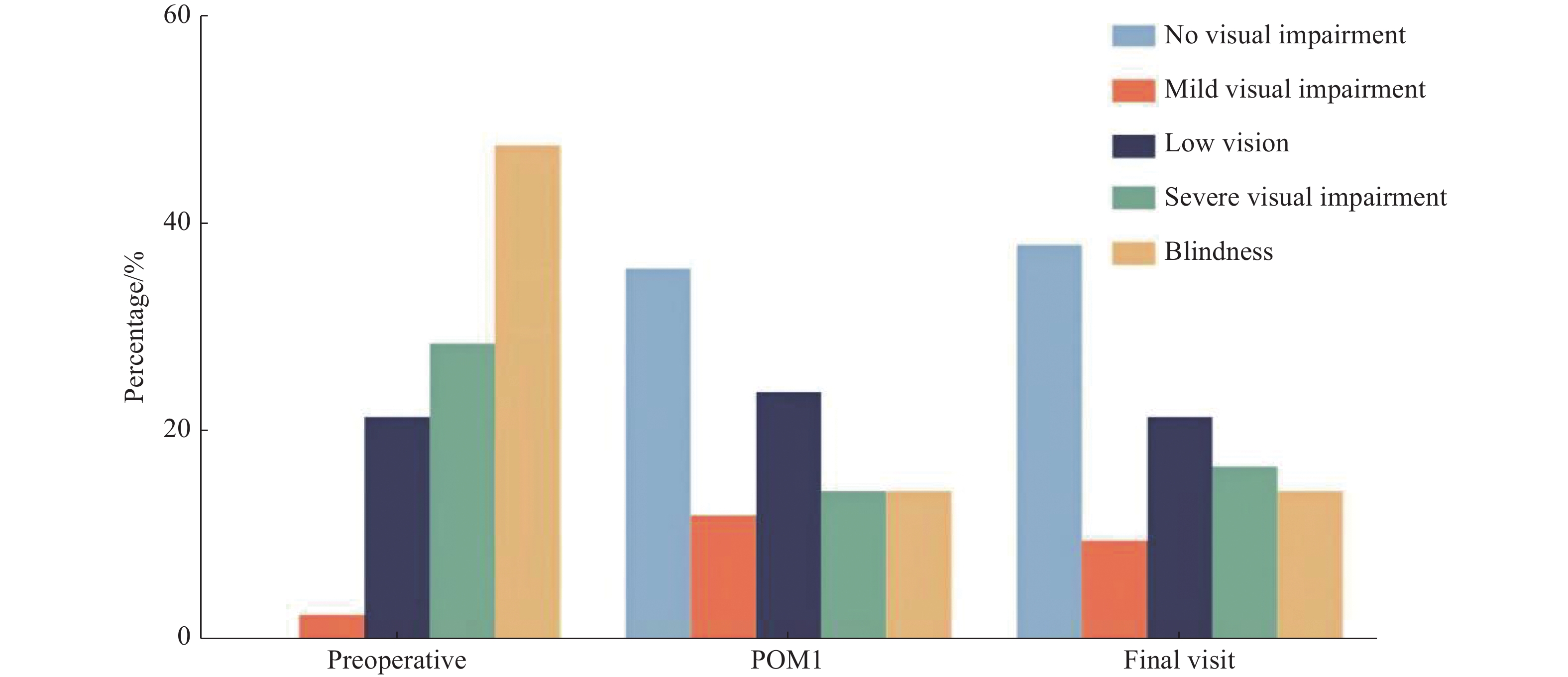
POM1: postoperative 1 month
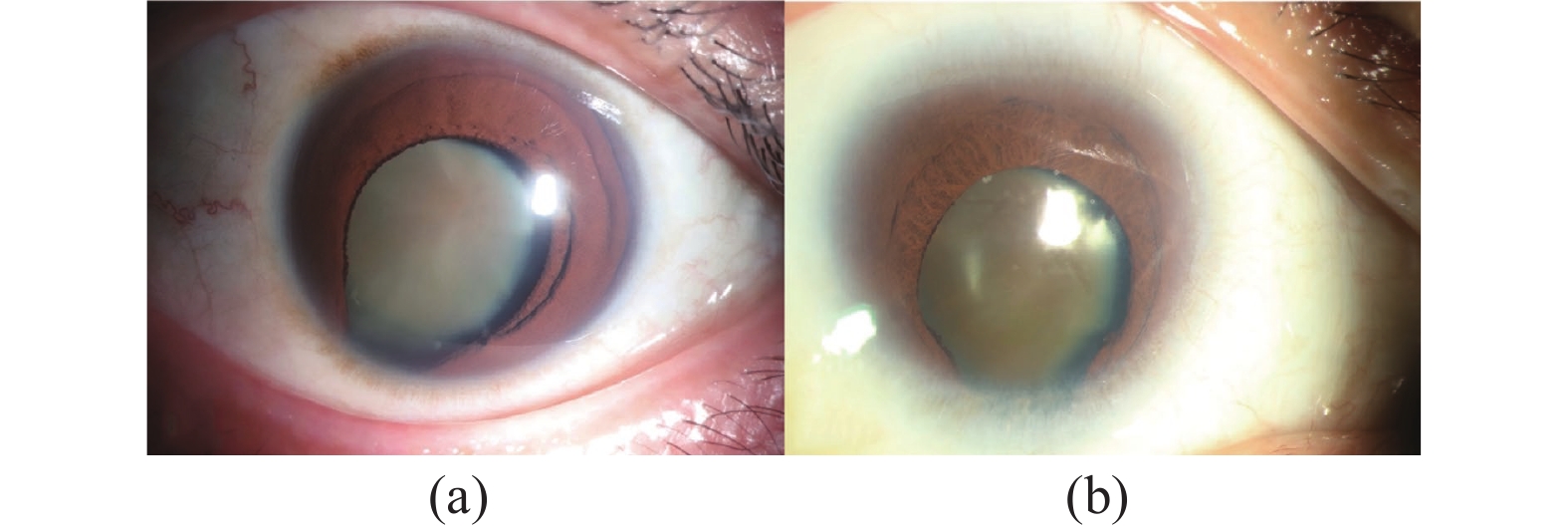
(a) A representative case of good visual outcome. This patient had a preoperative CDVA of 20/400, a corneal diameter of 11 mm, and postoperative CDVA of 20/32. (b) A representative case of poor visual outcome. This patient had a preoperative CDVA of counting finger, a corneal diameter of 8mm, and postoperative CDVA of 20/200.
|
Characteristic |
Univariate analysis |
Multivariable analysis |
||
|
OR (95% CI) |
P |
OR (95% CI) |
P |
|
|
Age (y) |
0.95 (0.89, 1.02) |
0.161 |
- |
|
|
Female |
0.79 (0.21, 3.07) |
0.729 |
- |
|
|
Preoperative CDVA (logMAR) |
11.19 (2.17, 57.77) |
0.004* |
16.01 (1.38, 185.40) |
0.026* |
|
IOP (mmHg) |
1.09 (0.84, 1.39) |
0.560 |
- |
|
|
AL (mm) |
1.16 (0.90, 1.48) |
0.247 |
- |
|
|
Microcornea |
16.80 (2.69, 104.82) |
0.003* |
18.65 (1.45, 240.52) |
0.025* |
|
Hard nuclear cataract |
6.25 (1.33, 29.43) |
0.020* |
0.77 (0.70, 8.97) |
0.837 |
|
Extent of iris coloboma |
3.17 (0.80, 1.39) |
0.236 |
- |
|
|
Strabismus |
0.66 (0.11, 3.97) |
0.645 |
- |
|
|
Nystagmus |
0.21 (0.55, 16.08) |
0.208 |
- |
|
|
CDVA: corrected distance visual acuity, IOP: intraocular pressure, AL: axial length. *Statistically significant. Poor postoperative visual prognosis is defined as postoperative CDVA < 1.0 logMAR. Analysis was performed using the first eye of each patient undergoing surgery. |
||||
Subgroup analysis based on fundus involvement
To further investigate the influence of non-fundus factors on postoperative visual prognosis, a subgroup analysis was performed among patients with (n=11) and without (n=31) optic disc or macula involvement Among eyes with coloboma involving the optic disc or macula, all had poor postoperative visual outcomes (CDVA > 1.0 logMAR). In the subgroup of eyes without optic disc or macula involvement, logistic regression analysis revealed that only age was significantly associated with poor postoperative visual outcomes (CDVA > 1.0 logMAR) (OR = 0.868, 95% CI: 0.757 to 0.995, P = 0.042).
Discussions
In this retrospective study, cataract surgery demonstrated significant efficacy in improving visual acuity in patients with congenital iridochoroidal coloboma. However, the safety of cataract surgery should be carefully considered, as the intraocular complication rate was 19.0%, with PCR and ZD being the most common complications. Multivariate logistic regression identified poor preoperative CDVA and microcornea as significant predictors of poor postoperative visual outcomes.
The most common type of cataract observed in this study was nuclear sclerosis, with a hard nuclear cataract rate of 47.6%, consistent with previous studies.8 The mean age at surgery was (45.4 ± 8.2) years, similar to that reported by Shekhar et al., but significantly higher than that reported by Sahay et al and Khokhar et al.[7-8,14] The rate of disc/macula involvement in our study was 23.8%, comparable to that reported by Phylactou et al. (19.5%) but lower than that reported by Shekhar et al. (46.2%).[8-9]
Iridochoroidal coloboma is frequently associated with other ocular structural abnormalities, which may increase the risk of intraoperative and postoperative complications. In this study, the incidence of intraoperative complications was 19.0%, including PCR in 2 eyes and ZD in 6 eyes. Previous studies have reported PCR rates ranging from 4% to 23% and ZD rates ranging from 2.4% to 40% during cataract surgery in eyes with coloboma.[7-8,14-16] Eyes with hard cataract and microcornea were more likely to experience intraoperative complications.[8,15] For high-risk eyes, particularly those with microcornea, shallow anterior chamber, or hard cataract, MSICS may be a more suitable approach than PE. Postoperatively, mild IOL dislocation occurred in 2 eyes and retinal detachment in 1 eye. Therefore, special attention should be given to the prevention and management of complications during and after cataract surgery in these patients.
In this study, CDVA showed significant improvement at 1 month postoperatively and at the final visit, with 69.0% of eyes demonstrating visual improvement. The postoperative CDVA (0.79 logMAR) in our series was comparable to that reported by Khokhar et al. (0.96 logMAR) but better than that results reported by Sahay et al. (1.64 logMAR) and Chaurasia et al. (1.51 logMAR).[7,14-15] These findings suggest that, even the elevated risk of complications, cataract surgery can provide substantial visual benefit.
However, 31.0% of eyes still had postoperative CDVA worse than 1.0 logMAR. This was largely attributable to coloboma involving the optic disc or macula, which leads to irreversible vision loss and limits the potential for visual improvement after cataract surgery. Notably, these eyes still experienced significant improvement compared with preoperative CDVA. Thus, surgery can be a reasonable option even in eyes with poor visual potential, provided patients are counseled appropriately.
To explore predictors of postoperative visual prognosis independent of fundus examination, we analyzed several preoperative factors. In the full series, poor preoperative CDVA and microcornea were significantly associated with poor postoperative visual outcomes. Preoperative CDVA may reflect both the severity of cataract and the extent of coloboma. Shekhar et al. observed that patients with hard cataract showed poor postoperative visual recovery compared with those with soft cataract, which could be attributed to the higher complication rates in hard cataract (36.9% vs. 25%).[8] However, in this study, hard cataract was not significantly associated with poor visual outcomes in multivariable logistic regression, consistent with Kohli, et al.’s findings.[16] Indeed, hard cataract may increase the risk of intraoperative complications (30% vs. 9% in current study), but it did not appear to be directly related to the postoperative visual prognosis. Therefore, special attention should be given to the patients with poor preoperative CDVA. Nonetheless, it is essential to recognize that even in patients with severe cataract and poor preoperative CDVA, there is still potential for visual improvement.
Our results also indicated an association between microcornea and poor visual outcomes. Similarly, Hornby et al.[17] and Tibrewal et al.[18] found that the presence of microcornea in patients with coloboma predicted worse vision outcomes. Mmicrocornea is often associated with a spectrum of ocular abnormalities, including ocular coloboma, congenital cataract, glaucoma, chorioretinal hypoplasia, and optic nerve aplasia.[19] We hypothesize that the microcornea may reflect more severe developmental and structural abnormalities within the eyes, such as advanced retinal dysplasia, contributing to poor visual outcomes. However, further research is necessary to confirm this hypothesis and explore the underlying mechanisms.
Furthermore, our findings indicated that patient age was not significantly associated with postoperative visual prognosis in the overall cohort. However, subgroup analysis provided more nuanced insights: among patients without optic disc or macular involvement, older age was significantly associated with worse postoperative visual outcomes. This suggests that age may become a more relevant prognostic factor when the confounding effect of fundus pathology is minimized. Previous studies have indicated that early cataract surgery in eyes with iridochoroidal coloboma may lead to better visual outcomes, with higher rates of uneventful surgeries, successful IOL implantation, and lower incidences of PCR.[8,15] In contrast, in the subgroup with optic disc or macular involvement, all patients exhibited poor postoperative visual acuity, regardless of age or other ocular characteristics. This confirms that central fundus abnormalities are a dominant determinant of visual prognosis. Although cataract surgery results in the loss of accommodative abilities of crystalline lens, it is crucial to recognize that early surgery may also yield better visual outcomes and reduce the risk of intraoperative complications. Therefore, further investigations are warranted to determine the optimal timing for cataract surgery in patients with iridochoroidal coloboma.
This study has several limitations. First, as a retrospective study, there are inherent concerns regarding selection bias. Second, the relatively sample size may restrict the generalizability of the findings. Further studies with a larger sample size are necessary to validate and extend the current observations. Third, long-term visual outcomes and complications were not investigated. Despite these limitations, given that iridochoroidal coloboma is a rare disease, the results provide valuable insights and supplement the existing literature.
In conclusion, timely and appropriate surgical intervention for the cataract in eyes with congenital iridochoroidal coloboma can effectively improve visual outcomes. Poor preoperative CDVA and the presence of microcornea were identified as important indicators of poor visual prognosis.
Correction notice
None
Acknowledgements
None
Author Contributions
(I) Conception and design: Shuxin Fan, Siyuan Liu, Shengsong Huang
(II) Administrative support: Xialin Liu, Shengsong Huang
(III) Provision of study materials or patients: Shengsong Huang, Danying Zheng
(IV) Collection and assembly of data: Siyuan Liu, Yimeng Zhang, Feiyan liang
(V) Data analysis and interpretation: Siyuan Liu
(VI) Manuscript writing: All authors
(VII) Final approval of manuscript: All authors
Conflict of Interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form.
Patient consent for publication
None
Ethics approval and consent to participate
None
Data availability statement
None
Open access
This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License(CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited(including links to both the formal publication through the relevant DOI and the license).