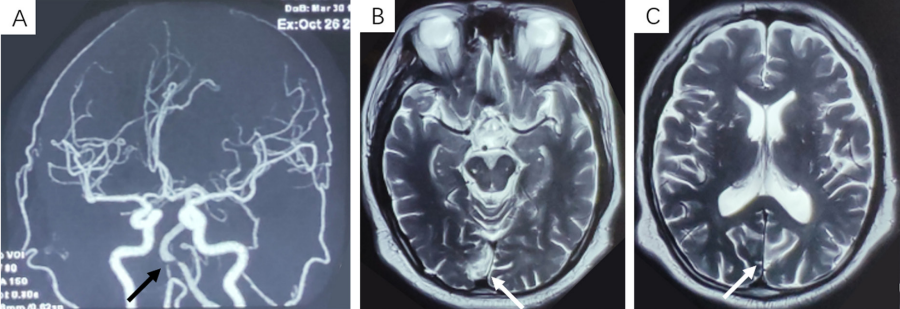
(A)Cranial vascular MRA shows the stenosis of basilar artery initial portion(black arrow); (B, C)Cranial MRI shows that T2 hyperintensity is seen in both occipital lobes and consistent with occipital infarction (white arrow).
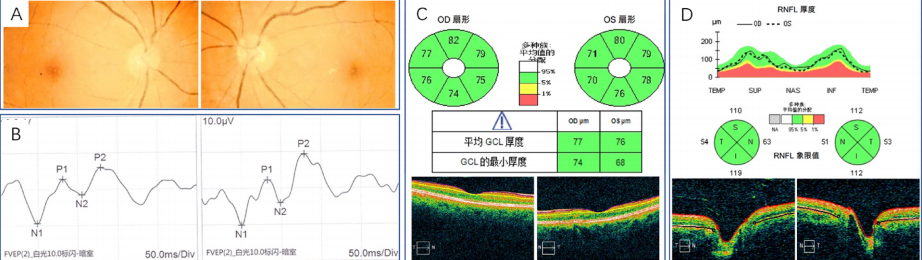
(A)Fundus color photo: Clear boundary of optic disc with good color in bilateral eyes; (B)The results of F-VEP showed that the peak of P2 wavewas delayed in bilateral eyes, and the peak of P2 wave in right eye was lower than that in left eye; (C, D) OCT examination showed no obvious abnormalities in RNFL of optic disc and ganglion cells of macular area.
图3 双眼24-2及10-2 Humphrey自动视野检查
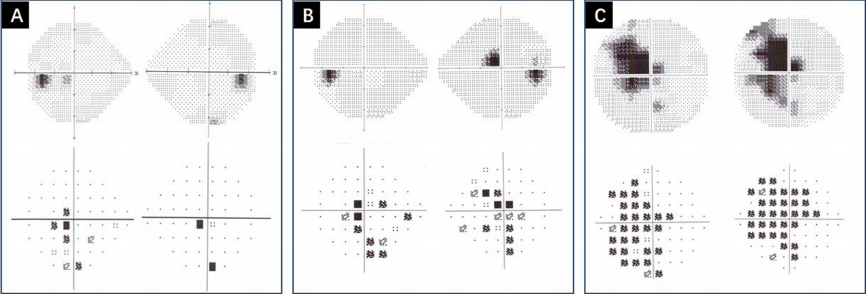
Figure 3 24-2 and 10-2 program Humphrey automatic visual field examination of bilateral eyes
24-2 program Humphrey automatic visual field examination(upward: grey-scale plot; downward: pattern deviation plot): A: central field scotoma in left eye(homonymous scotoma tendency, September 1, 2020), B: central scotoma in right eye (in superior nasal visual field, and several scotomas in bilateral eyes with unclear tendency, February 14, 2022); 10-2 program Humphrey automatic visual field examination: C: left homonymous hemianopia; (homonymous scotoma, February 14, 2022).
图4 头颅MRI检查
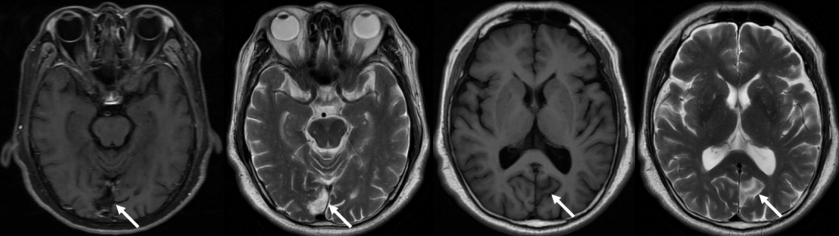
Figure 4 Cranial magnetic resonance imaging
头颅MRI(2022-0218)提示:双侧枕叶梗死(箭头)。
Cranial magnetic resonance imaging(February 18, 2022): Infarction of bilateral occipital lobe(arrow).
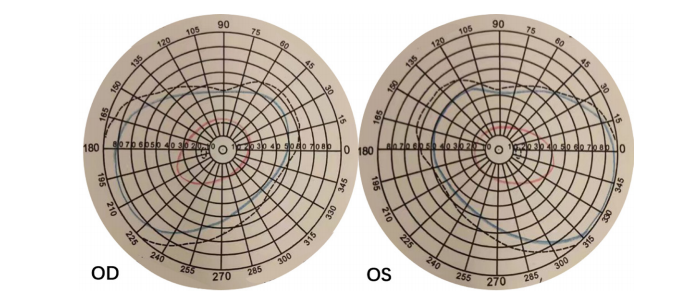
图5 Goldmann动态视野检查
Figure 5 Goldmann kinetic perimeter
Goldmann动态视野检查提示:右眼颞侧新月状视野缺损。
Goldmann kinetic perimeter: Visual field defect of temporal crescent of right eye.
1. 国家自然科学基金青年项目(82101110)。 This work was supported by the National Natural Science Foundation of China
(82101110).
参考文献
1. Fahrenthold BK, Cavanaugh MR, Jang S, et al. Optic tract shrinkage
limits visual restoration a er occipital stroke[ J]. Stroke, 2021, 52(11):
3642-3650.
2. Koch G, Bonnì S, Giacobbe V, et al. θ-burst stimulation of the left
hemisphere accelerates recovery of hemispatial neglect[ J]. Neurology,
2012, 78(1): 24-30.
3. de Haan GA, Heutink J, Melis-Dankers BJ, et al. Spontaneous recovery
and treatment effects in patients with homonymous visual field defects:
a meta-analysis of existing literature in terms of the ICF framework[ J].
Surv Ophthalmol, 2014, 59(1): 77-96.
4. Zhang X, Kedar S, Lynn M J, et al. Natural history of homonymous
hemianopia[ J]. Neurology, 2006, 66(6): 901-905.
5. R afique SA , Richards JR , Steeves JKE. Altered white matter
connectivity associated with visual hallucinations following occipital
stroke[ J]. Brain Behav, 2018, 8(6): e01010.
6. Morenas-Rodríguez E, Camps-Renom P, Pérez-Cordón A, et al. Visual
hallucinations in patients with acute stroke: a prospective exploratory
study[ J]. Eur J Neurol, 2017, 24(5): 734-740.
7. Galletti C, Fattori P. The dorsal visual stream revisited: stable circuits or
dynamic pathways?[ J]. Cortex, 2018, 98: 203-217.
8. Kwan WC, Chang CK, Yu HH, et al. Visual cortical area MT is required
for development of the dorsal stream and associated visuomotor
behaviors[ J]. J Neurosci, 2021, 41(39): 8197-8209.
9. Murray MM, Thelen A, Thut G, et al. The multisensory function of the
human primary visual cortex[ J]. Neuropsychologia, 2016, 83: 161-169.
10. Zachariou V, Klatzky R, Behrmann M. Ventral and dorsal visual stream
contributions to the perception of object shape and object location[ J].
J Cogn Neurosci, 2014, 26(1): 189-209.
11. Kartsounis LD, James-Galton M, Plant GT. Anton syndrome,
with vivid visual hallucinations, associated with radiation induced
leucoencephalopathy[ J]. J Neurol Neurosurg Psychiatry, 2009, 80(8):
937-938.
12. Horton JC, Economides JR, Adams DL. The mechanism of macular
sparing[ J]. Annu Rev Vis Sci, 2021, 7: 155-179.
13. Mehra D, Moshirfar M. Neuroanatomy, Optic Tract. Treasure Island
(FL): StatPearls Publishing, 2022.
14. Kardon R, Kawasaki A, Miller NR. Origin of the relative afferent
pupillary defect in optic tract lesions[ J]. Ophthalmology, 2006,
113(8): 1345-1353.
15. Short RA, Graff-Radford N R. Localization of Hemiachromatopsia[ J].
Neurocase, 2001, 7(4): 331-337.
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)