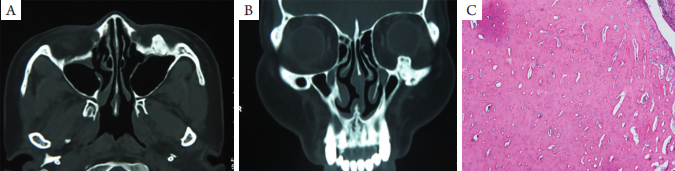
(A) Horizontal CT showed the increased density of the left inferior orbital wall with uniform density and obvious edge. The edge of the tumor was regular, without dissolution and destruction; (B) Coronal CT showed high-density shadow of the infraorbital wall, protruding into the orbit and squeezing the eyeball; (C) A small amount of fibrous connective tissue and bone trabeculae were seen under the microscope (HE, ×5).
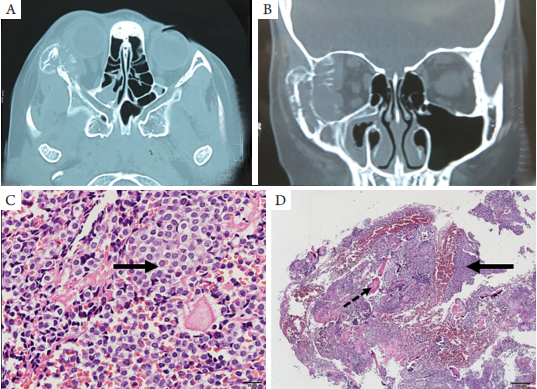
图2 骨内血管瘤CT图像和病理学表现
Figure 2 CT images and pathological findings of intraosseous hemangioma
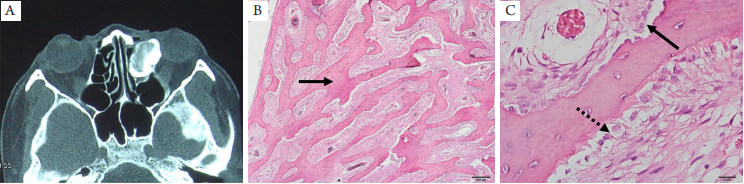
(A) CT image of patient 1: The swelling growth tumor shadow of the right cheekbone is palisade like and honeycomb like mixed density shadow. The internal density is uneven, and thick bone ridge shadow can be seen; (B) Pathological results of patient 1: Vascular structures (thick and thin arrows) with different lumen sizes can be seen between trabeculae (dotted arrows); (C) CT image of patient 2: right orbital bone mass, mixed high and low density; (D) Pathological results of case 2: The thin arrow points to periosteum; the dotted arrow points to osteoid matrix, and the thick arrow points to the spongy cavernous hemangioma structure between trabeculae (HE, ×5).
图3 骨样骨瘤眼眶CT图像和病理学表现
Figure 3 CT images and pathological findings with the orbit of osteoid osteoma
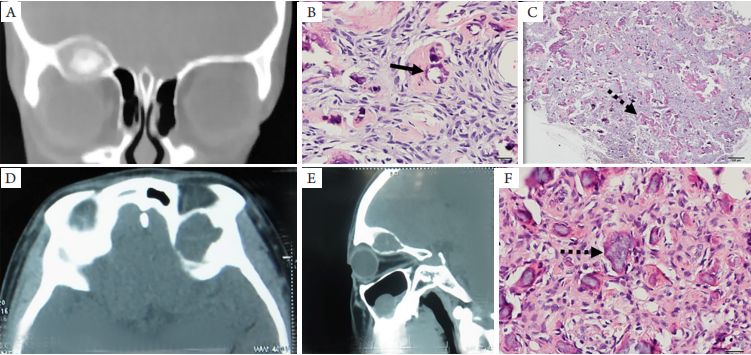
(A) Mass mixed density shadow in the left ethmoid sinus mass, dense sclerotic bone cortex surrounding a radiolucent "tumor nest", and growing in the left orbit, with bone discontinuity in the left orbital wall. Peripheral bone sclerosis images with increased density, uniform density, obvious edge, no dissolution, and no destruction; (B) Pathological results showed that the tumor tissue was composed of bone cells and osteoid matrix, containing fibrous tissue and osteoid trabeculae. The arrow points to trabeculae (HE, ×5); (C) The solid line arrow points to osteoclasts and the dotted arrow points to osteoblasts (HE, ×40).
图4 骨化纤维瘤眼眶CT图像和病理学表现
Figure 4 CT images and pathological results of ossifying fibroma
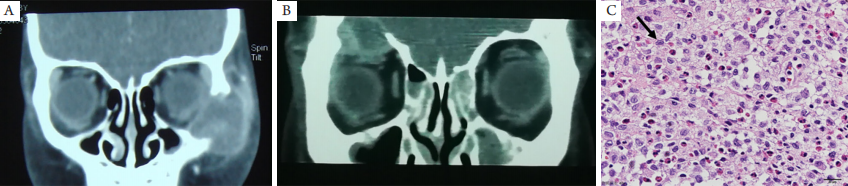
(A) Patient 1: Coronal CT shows irregular shape and well-defined mass in the left orbital bone, showing heterogeneous medium and high-density soft tissue mass with bone components, which are closely related to bone wall defect; (B) Patient 2: Coronal CT shows irregular, well-defined mass in the right frontal bone, heterogeneous medium and high-density soft tissue mass with high-density shadow in the mass; (C) A large number of Langerhans cells can be seen (solid arrow) with diffuse eosinophils and a small number of small lymphocytes infiltration (HE, ×40).
图6 尤文肉瘤眼眶CT图像和病理学表现
Figure 6 CT images and pathological findings of Ewing’s sarcoma
(A) Horizontal CT showed osteolysis and destruction of the zygomatic process of the right maxilla, and the lesion involved the great wing of sphenoid bone backward; (B) Coronal CT showed that the lesion extended upward to the frontal bone and downward to the wall of maxillary sinus, with radial bone needle formation. The tumor penetrated through the bone cortex to form a soft tissue density mass, which bulged into the orbit and pushed the eyeball and orbital tissue to the medial side; (C, D) Small round cell tumor (solid arrow) with round nucleus, fine chromatin, and small nucleoli (HE, ×40); (D) Bone trabeculae between tumor cells (dotted arrow) (HE, ×5).
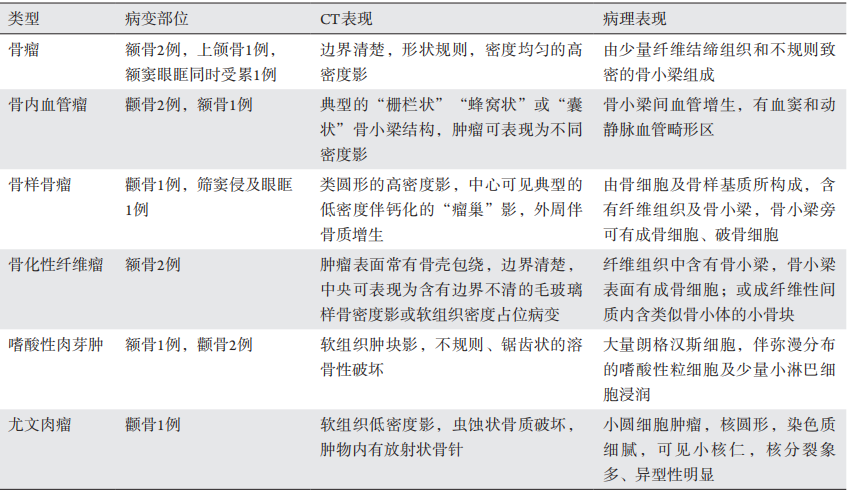
表1 发生于眶骨的占位性病变影像及病理结果
Table 1 Imaging and pathological results of space occupying lesions in orbital b
1. 天津市临床重点学科建设项目 (TJLCZDXK7006)。 This work was supported by Tianjin Clinical Key Discipline
Construction Project, China (TJLCZDXK7006).
参考文献
1. Selva D, White VA, O’Connell JX, et al. Primary bone tumors of the
orbit[ J]. Surv Ophthalmol, 2004, 49(3): 328-342.
2. Mchugh JB, Mukherji SK , Lucas DR . Sino-orbital osteoma: a
clinicopathologic study of 45 surgically treated cases with emphasis
on tumors with osteoblastoma-like features[ J]. Arch Pathol Lab Med,
2009, 133(10): 1587-1593.
3. Soni S, Bhargava A. Revisiting peripheral osteoma of the mandible with
case series and review of literature[ J]. Indian J Otolaryngol Head Neck
Surg, 2014, 66(2):212.
4. 丁宜, Bui Marilyn, 孙晶,等. 单中心107例骨原发血管源性肿瘤临
床病理分析[ J]. 临床与实验病理学杂志, 2016, 32(7): 766-769.
DING Y, BUI Marilyn, SUN J, et al. Primary vascular tumors of
bone: clinicopathologic analysis of 107 patients from single center
institution[ J]. Chinese Journal of Clinical and Experimental Pathology,
2016, 32(7): 766-769.
5. Brandner JS, Rawal YB, Kim LJ, et al. Intraosseous hemangioma of the
frontal bone. Report of a case and review of the literature[ J]. J Oral
Maxillofac Surg, 2017, 76(4): 799-805.
8. Deferm JT, Sca S, Vriens D, et al. Chronic temporomandibular joint
pain: two cases of osteoid osteoma and a review of the literature[ J]. Int
J Oral Maxillofac Surg, 2017, 46(9): 1130-1137.
9. The usefulness of chemical-shift magnetic resonance imaging for the
evaluation of osteoid osteoma[J]. Radiologia Brasileira, 2018, 51(3):156-161.
10. Figueiredo LM, de Oliveira TF, Paraguassú GM, et al. Psammomatoid
juvenile ossifying fibroma: case study and a review[ J]. Oral Maxillofac
Surg, 2014, 18(1): 87-93.
11. Khanna M, Buddhavarapu SR, Hussain SA, et al. Cemento-ossifying
fibroma of paranasal sinus presenting acutely as orbital cellulitis[ J]. J
Radiol Case Rep, 2009, 3(4): 18-25.
12. 杨秀萍, 龚树生. 8例青少年鼻窦骨化性纤维瘤的临床病理观
察[ J]. 中国临床医学, 2003, 10(5): 693-694.
YANG XP, GONG SS. Clinicopathologic observation
of the juvenile ossifying fibromas of paranasal sinuses in 8 cases[ J].
Clinical Medical Journal of China, 2003, 10(5): 693-694.
13. Barnes L, Eveson JW, Reichart P, et al. Pathology and genetics of head
and neck tumors[M]. Geneva: WHO Press, 2006.
14. Kawaguchi M, Kato H, Miyazaki T, et al. CT and MR imaging
characteristics of histological subtypes of head and neck ossifying
fibroma[ J]. Dentomaxillofac Radiol, 2018, 47(6): 20180085.
15. 李学锋, 戴芳, 赵玺龙, 等. 青少年沙瘤样骨化纤维瘤临床病理分
析[ J]. 临床与实验病理学杂志, 2011, 27(8): 888-890.
LI XF, DAI F, ZHAO XL, et al. Clinicopathological
analysis of juvenile psammomatoid ossifying fibroma[ J]. Chinese
Journal of Clinical and Experimental Pathology, 2011, 27(8):888-890.
16. 段瑞. WHO造血与淋巴组织肿瘤分类(2016)[ J]. 诊断病理学杂
志, 2017, 24(12): 956-958.
DUAN R. WHO classification of hematopoietic and lymphoid
tumors (2016)[ J]. Chinese Journal of Diagnostic Pathology, 2017,
24(12): 956-958.
17. Kitsoulis PV, Paraskevas G, Vrettakos A, et al. A case of eosinophilic
granuloma of the skull in an adult man: a case report[ J]. Cases J, 2009,
2(1): 9144.
18. 李振武, 李天云, 解非, 等. 尤文肉瘤的影像学诊断[ J]. 现代肿瘤
医学, 2015(23): 3474-3477.
LI ZW, LI TY, XIE F, et al. Value of imaging in the
diagnosis of Ewing’s sarcoma[ J]. Journal of Modern Oncology,
2015(23): 3474-3477.
19. Somarouthu BS, Shinagare AB, Rosenthal MH, et al. Multimodality
imaging features, metastatic pattern and clinical outcome in adult extra
skeletal Ewing sarcoma: experience in 26 patients[ J]. Br J Radiol, 2014,
87(1038): 20140123.
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)