Subclinical inflammatory response after accelerated corneal cross-linking
阅读量:1350
DOI:doi: 10.3978/j.issn.1000-4432.2016.06.05
发布日期:2024-11-29
作者:
Hassan Hashemi ,Nahid Ashraf ,Ebrahim Jafarzadehpur ,Alireza Hedayatfar
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Keratoconus
accelerated cross-linking
clinical trial
inflammation
摘要
Background: To evaluate the inflammatory response after accelerated collagen cross-linking (CXL) in
eyes with keratoconus.
Methods: Consecutive eyes with keratoconus undergoing CXL surgery were included in this nonrandomized
interventional study. Aqueous flare was measured pre- and post-operatively with a laser flare
photometer at 1 week, 1, 3 and 6 months after CXL.
Results: Sixty eyes of 60 patients were entered into the study. Before CXL, the mean flare value was
4.5 photons per millisecond (ph/ms). The flare values observed at week 1 (7.1 ph/ms; P=0.008), month 1
(6.5 ph/ms; P=0.04), month 3 (6.7 ph/ms; P=0.004) and month 6 (6.7 ph/ms; P=0.004) were significantly
higher compared to baseline. Flare values were not significantly different from week 1 up to 6 months
after CXL (P=0.930). No statistically significant correlation was detected between the amount of
inflammation and keratometric indices.
Conclusions: Accelerated CXL in patients with keratoconus may cause a subclinical inflammatory
response which is evident as slight but rather long-lasting rise of aqueous flare.
全文
Introduction
Corneal collagen cross-linking (CXL) is a recognized
technique for slowing or halting the progression of
keratoconus using riboflavin and UV light which results in
corneal strengthening through the formation of covalent
bonds in the corneal stroma. In the standard technique
described by Wollensak et al., the riboflavin-treated eye
is illuminated for 30 minutes by UVA 370 nm light at an
irradiance of 3 mW/cm2
(cumulative dose 5.4 J/cm2
) (1).
Today, there is growing interest in the accelerated approach
in which the procedure time is reduced by increasing the
irradiation power and decreasing the exposure time (2-4).
Prior studies have shown a significant short-term rise of
aqueous flare following refractive photo ablative surgeries
with or without lamellar keratectomy (5-8). In this study we
aimed to evaluate flare as an indicator of the inflammatory
response following accelerated CXL.
Patients with mild to moderate keratoconus [maximum K less than 55 diopters (D)] and the following inclusion criteria were enrolled: (I) age between 18 and 35 years; (II) best-corrected visual acuity (BCVA) of 20/40 or worse; (III) topographic evidence of progressive keratoconus defined as ≥1.0 D increase in maximum keratometry and/or the manifest cylinder, or ≥0.5 D increase in refraction spherical equivalent over 24 months (3); (IV) minimum corneal thickness of 450 µm. Patients with a history of prior ocular surgeries, inflammatory ocular or systemic disease (e.g., diabetes) and recent contact lens usage were not enrolled.
Before CXL, all eyes underwent complete ophthalmic examinations including measurement of uncorrected visual acuity (UCVA) and BCVA, slit-lamp biomicroscopy and fundus examination, corneal Scheimpflug imaging (Pentacam, OCULUS, Inc., Lynnwood, WA, USA) and laser flare photometry (FM-600; Kowa, Tokyo, Japan). All examinations were repeated at 1 week, 1, 3, and 6 months after CXL.
Methods
This prospective, non-randomized interventional beforeafter study was performed at Noor Eye Hospital, Tehran. All patients, enrolled from September 2012 to January 2013, were informed, and consent was obtained after the procedure had been explained. The study protocol was approved by the Institutional Review Board of Noor Ophthalmology Research Center (IRB# M.1118).Patients with mild to moderate keratoconus [maximum K less than 55 diopters (D)] and the following inclusion criteria were enrolled: (I) age between 18 and 35 years; (II) best-corrected visual acuity (BCVA) of 20/40 or worse; (III) topographic evidence of progressive keratoconus defined as ≥1.0 D increase in maximum keratometry and/or the manifest cylinder, or ≥0.5 D increase in refraction spherical equivalent over 24 months (3); (IV) minimum corneal thickness of 450 µm. Patients with a history of prior ocular surgeries, inflammatory ocular or systemic disease (e.g., diabetes) and recent contact lens usage were not enrolled.
Before CXL, all eyes underwent complete ophthalmic examinations including measurement of uncorrected visual acuity (UCVA) and BCVA, slit-lamp biomicroscopy and fundus examination, corneal Scheimpflug imaging (Pentacam, OCULUS, Inc., Lynnwood, WA, USA) and laser flare photometry (FM-600; Kowa, Tokyo, Japan). All examinations were repeated at 1 week, 1, 3, and 6 months after CXL.
Surgical technique
The eye was anesthetized by instillation of one drop
of tetracaine hydrochloride 0.5% (Anestocaine 0.5%,
Sina-Darou Pharm. Co., Tehran, Iran). After removal
of the epithelium from the central 7 mm of the cornea,
0.1 mL of riboflavin 0.1% in dextran solution 20%
(Streulipharmeceuticals, Uznach, Switzerland) was
instilled onto the cornea every 3 minutes for a total time
of 30 minutes. Accelerated CXL was performed using
5 minutes of continuous UVA 370 nm light (IROC UVX
system, Zürich, Switzerland) at an irradiance of 18 mW/cm2
(cumulative dose 5.4 J/cm2
). A therapeutic soft contact lens
(Night & Day, Ciba Vision, Duluth, GA, USA) was fitted
at the end of the procedure. All patients were treated postoperatively
with levofloxacin 0.5% and betamethasone
0.1% 4 times daily for 1 week and were examined daily
until complete healing of the epithelium when the bandage
contact lenses were removed.
Anterior chamber flare measurement
Anterior chamber flare was measured with a regularly
calibrated laser flare photometer (FM-600, Kowa, Tokyo, Japan). For each eye, seven consecutive readings were
obtained from the lower third of the anterior chamber
with <10% background scatter. The two extreme readings
were crossed out, and the average of the remaining five was
recorded as the flare value in photons per millisecond (ph/ms).
Statistical analysis
Statistical analysis was performed using the repeated
measures analysis of variance to compared results of the
pre- and postoperative examinations. For the analysis of
associations between quantitative variables, the Pearson
correlation test was applied. A P value <0.05 was considered
statistically significant.
Results
Sixty eyes of 60 patients with mild to moderate keratoconus
were entered into this study. Mean age of the patients
was 23.8 years (range, 15−35 years). Before CXL, their
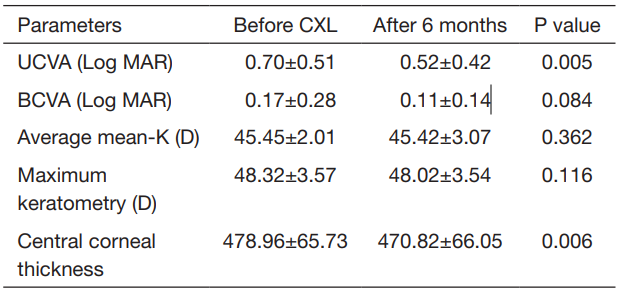
mean UCVA was 0.71±0.51 logMAR and improved to
0.52±0.42 logMAR 6 months after surgery (P=0.039).
Mean BCVA was also improved from 0.17±0.28 logMAR
preoperatively to 0.11±0.14 logMAR 6 months after surgery
(P=0.011). Table 1 summarizes clinical profiles before CXL
and 6 months after the procedure.
The mean anterior chamber flare increased from 4.5 ph/ms before CXL to 7.1±7.5 ph/ms 1 week post-operatively (P=0.008). Although the mean flare value decreased slightly to 6.5±4.8 ph/ms at 1 month, it was still significantly higher than baseline (P=0.040). The changes were rather steady from month 1 up to the last visit (Figure 1). There were no statistically significant differences between mean flare values at week 1 and other follow-up visits.
 UCVA, uncorrected visual acuity; BCVA, best-corrected visual
acuity; CXL, collagen cross-linking.
UCVA, uncorrected visual acuity; BCVA, best-corrected visual
acuity; CXL, collagen cross-linking.
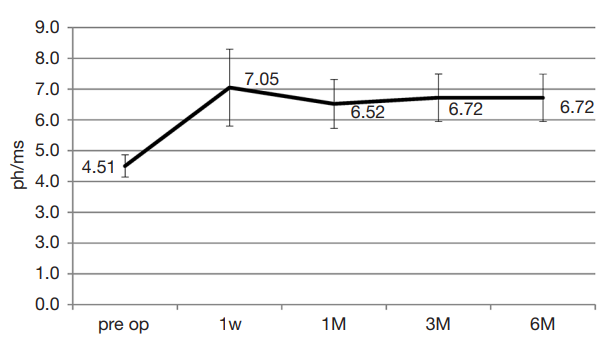
The mean anterior chamber flare increased from 4.5 ph/ms before CXL to 7.1±7.5 ph/ms 1 week post-operatively (P=0.008). Although the mean flare value decreased slightly to 6.5±4.8 ph/ms at 1 month, it was still significantly higher than baseline (P=0.040). The changes were rather steady from month 1 up to the last visit (Figure 1). There were no statistically significant differences between mean flare values at week 1 and other follow-up visits.
Table 1 Patients’ clinical profiles at baseline and 6 months after accelerated corneal collagen cross linking
Figure 1 Mean anterior chamber flare with corresponding error bar depicting 95% confidence interval before, 1 week, 1, 3 and 6 months after CXL. ph/ms, photons per millisecond; CXL, collagen cross-linking.
Discussion
The postoperative inflammatory response remains an
important determinant of corneal wound healing. Laser
flare meters allow for the quantification of the inflammatory
response through objective measurement of the aqueous
flare. With a high degree of accuracy and sensitivity, laser
flare meters can detect minute alterations in the bloodaqueous-barrier
function which may not be clinically
detectable (9).
Previous studies have shown the induction of an inflammatory response following photo ablative refractive surgeries. Tomas-Barberan and Fagerholm described a significant increase in anterior chamber flare after photorefractive keratectomy (PRK) (5). Others reported a short-lasting subclinical inflammation following uneventful laser in situ keratomileusis in virgin eyes (6) as well as corneal grafting (7). Pisella et al. showed that photo ablative refractive surgery with or without lamellar keratectomy could induce alteration in flare which is correlated with the depth of ablation (8).
In our study, following the accelerated CXL with UVA light at an irradiance of 18 mW/cm2 , an early and rather steady increase of aqueous flare occurred. Contrary to previous reports, the rise of aqueous flare was not shortterm and flare intensity did not return to baseline even up to 6 months after CXL. We speculate that the production of inflammatory mediators may have a causative role for this observation. During CXL, riboflavin molecules absorb the UVA light. In the presence of oxygen, a photo-oxidative reaction occurs and results in the excitation of riboflavin into a triplet state and generation of singlet oxygen. Excited riboflavin and oxygen free radicals catalyze biochemical reactions which result in the formation of additional covalent bonds between collagen fibers. The biochemical reaction and release of free radicals, as well as apoptosis of keratocytes lead to the local production of inflammatory cytokines which will subsequently affect the bloodaqueous-barrier function. Prior studies have shown that both mechanical and photochemical keratectomy produce inflammatory mediators such as PGE2, an observation that supports a role for cyclo-oxygenase inhibitors in postoperative therapy (10,11).
Previous studies have shown the induction of an inflammatory response following photo ablative refractive surgeries. Tomas-Barberan and Fagerholm described a significant increase in anterior chamber flare after photorefractive keratectomy (PRK) (5). Others reported a short-lasting subclinical inflammation following uneventful laser in situ keratomileusis in virgin eyes (6) as well as corneal grafting (7). Pisella et al. showed that photo ablative refractive surgery with or without lamellar keratectomy could induce alteration in flare which is correlated with the depth of ablation (8).
In our study, following the accelerated CXL with UVA light at an irradiance of 18 mW/cm2 , an early and rather steady increase of aqueous flare occurred. Contrary to previous reports, the rise of aqueous flare was not shortterm and flare intensity did not return to baseline even up to 6 months after CXL. We speculate that the production of inflammatory mediators may have a causative role for this observation. During CXL, riboflavin molecules absorb the UVA light. In the presence of oxygen, a photo-oxidative reaction occurs and results in the excitation of riboflavin into a triplet state and generation of singlet oxygen. Excited riboflavin and oxygen free radicals catalyze biochemical reactions which result in the formation of additional covalent bonds between collagen fibers. The biochemical reaction and release of free radicals, as well as apoptosis of keratocytes lead to the local production of inflammatory cytokines which will subsequently affect the bloodaqueous-barrier function. Prior studies have shown that both mechanical and photochemical keratectomy produce inflammatory mediators such as PGE2, an observation that supports a role for cyclo-oxygenase inhibitors in postoperative therapy (10,11).
The rise of aqueous flare following CXL may be
attributed in part to the surgical trauma to corneal tissue
secondary to epithelial removal. However, the same surgical
trauma during PRK only causes a temporary rise of aqueous
flare (5,8). Therefore, the rather long-term rise of flare
could not be attributed to the surgical trauma and hence,
the causative role of UVA irradiance in disrupting the
blood-aqueous barrier function is a more likely explanation.
Another possible explanation for the increased aqueous
haze would be the haze induced by CXL. Greenstein et al. (12) demonstrated that haze reaches a maximum at
the first month after CXL, remains relatively stable until
the third month, and takes a downward trend afterwards
to the 12th month. The postoperative formation of new
covalent bonds and corneal stromal changes can be another
reason for this subclinical inflammation. However, the
inflammation didn’t cause the clinical complications
and VA was significantly improved at this time as well.
Several studies have demonstrated the safety and efficacy
of CXL with the standard (13,14) and accelerated (2,15-17) approaches. There is no similar study on cases receiving
standard CXL, therefore, it is not clear whether lower
irradiance of UVA in standard CXL procedure will induct
such an inflammatory response or not. A limitation of
this stay was the short follow-up time. Also, studying
inflammatory changes in a non-operated group of
keratoconus patients would allow for a more accurate
conclusion about CXL-related changes in flare. Further
studies and longer follow-ups are needed.
Conclusions
In conclusion, the employment of higher fluence CXL
with shorter exposure time has recently been proposed as
an alternative to standard CXL technique in stabilizing keratoconus. Our study shows that the procedure may cause
a subclinical inflammatory response which is evident as
slight but a rather long-lasting rise of aqueous flare.
基金
暂无基金信息
参考文献
1. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultravioleta-inducedcollagen crosslinking for the treatment of keratoconus. Am J Ophthalmol 2003;135:620-7.
2. Kanellopoulos AJ. Long term results of a prospective randomized bilateral eye comparison trial of higher fluence, shorter duration ultraviolet A radiation, and riboflavin collagen cross linking for progressive keratoconus. Clin Ophthalmol 2012;6:97-101.
3. Celik HU, Alagöz N, Yildirim Y, et al. Accelerated corneal crosslinking concurrent with laser in situ keratomileusis. J Cataract Refract Surg 2012;38:1424-31.
4. Mrochen M. Current status of accelerated corneal crosslinking.Indian J Ophthalmol 2013;61:428-9.
5. Tomas-Barberan S, Fagerholm P. Anterior chamber flare after photorefractive keratectomy. J Refract Surg 1996;12:103-7.
6. El-Harazi SM, Chuang AZ, Yee RW. Assessment of anterior chamber flare and cells after laser in situ keratomileusis. J Cataract Refract Surg 2001;27:693-6.
7. Sen HN, Uusitalo R, Laatikainen L. Subclinical inflammation after laser in situ keratomileusis in corneal grafts. J Cataract Refract Surg 2002;28:782-7.
8. Pisella PJ, Albou-Ganem C, Bourges JL, et al. Evaluation of anterior chamber inflammation after corneal refractive surgery. Cornea 1999;18:302-5.
9. Shah SM, Spalton DJ, Smith SE. Measurement of aqueous cells and flare in normal eyes. Br J Ophthalmol 1991;75:348-52.
10. Szerenyi KD, Campos M, McDonnell PJ. Prostaglandin E2 production after lamellar keratectomy and photorefractive keratectomy. J Refract Corneal Surg 1994;10:413-6.
11. Phillips AF, Szerenyi K, Campos M, et al. Arachidonic acid metabolites after excimer laser corneal surgery. Arch Ophthalmol 1993;111:1273-8.
12. Greenstein SA, Fry KL, Bhatt J, et al. Natural history of corneal haze after collagen crosslinking for keratoconus and corneal ectasia: Scheimpflug and biomicroscopic analysis. J Cataract Refract Surg 2010;36:2105-14.
13. Hashemi H, Seyedian MA, Miraftab M, et al. Corneal collagen cross-linking with riboflavin and ultraviolet a irradiation for keratoconus: long-term results. Ophthalmology 2013;120:1515-20.
14. Vinciguerra R, Romano MR, Camesasca FI, et al. Corneal cross-linking as a treatment for keratoconus: four-year morphologic and clinical outcomes with respect to patient age. Ophthalmology 2013;120:908-16.
15. Hashemi H, Fotouhi A, Miraftab M, et al. Short-term comparison of accelerated and standard methods of corneal collagen crosslinking. J Cataract Refract Surg 2015;41:533-40.
16. Hashemi H, Miraftab M, Seyedian MA, et al. Longterm Results of an Accelerated Corneal Cross-linking Protocol (18 mW/cm2) for the Treatment of Progressive Keratoconus. Am J Ophthalmol 2015;160:1164-1170.e1.
17. Seiler TG, Fischinger I, Koller T, et al. Customized Corneal Cross-linking: One-Year Results. Am J Ophthalmol 2016;166:14-21.
相关文章
Honghe Xia;Riping Zhang;Alvin L. Young;Mingzhi Zhang,Long term changes of posterior corneal elevation after myopic laser in situ keratomileusisFereshteh Shokrollahzadeh;Hassan Hashemi;Ebrahim Jafarzadehpur;Ali Mirzajani;Mehdi Khabazkhoob;Soheila Asgari,Corneal biomechanics after rigid gas permeable contact lens wear in keratoconus eyes
Zhenggen Wu;Chukai Huang;Ce Zheng; Yuqiang Huang;Wanqi Zhang; Di Ma,The safety and effi cacy of modifi ed minimally invasive trabeculectomy for the treatment of primary chronic angle-closure glaucoma