Bilateral lens subluxation in a case of Behcet’s disease related uveitis
阅读量:1298
DOI:doi: 10.3978/j.issn.1000-4432.2016.09.01
发布日期:2024-12-01
作者:
Anubha Rathi ,Brijesh Takkar
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
摘要
全文
Ocular inflammation accompanying the pediatric Behcet’s
disease (BD) is characterized by a relapsing and complicated
course, often resulting in blindness due to severe bilateral
affection (1). Ectopia lentis (EL) is an important association
of multiple ocular and systemic syndromes, with favorable
visual outcomes if managed ideally (2). We discuss a unique
case presenting with a combination of these entities, and
explore the possible causes.
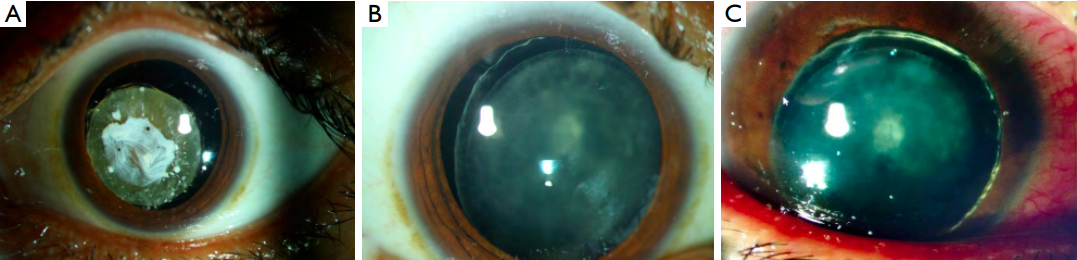
A 20-year-old male presented to our clinic with severe vision loss since 10–12 years of age, along with history of recurrent redness and pain in early childhood that was managed with topical and oral steroids as per old documents. There were definite history and signs of multiple apthosis; oral as well as genital; along with positivity for HLA B5, but no significant family history or mental disability. The vision loss had become more severe in the past few years with present corrected visual acuity being hand motions close to face OU. OU subluxation of the lens was noted, OS having dense absorbed cataract with capsular fibrosis while OD had complicated posterior subcapsular cataract (Figure 1). There were also signs of previous panuveitis OU, with few old keratic precipitates in both the eyes accompanied by severe sclerosing mixed retinal vasculitis, maculopathy and optic atrophy (Figure 2). Intra ocular pressure (IOP) was normal OU. Serum Treponemal antibody tests were negative and urine examination was negative for amino aciduria. Marfan’s syndrome was ruled out with Echocardiography. The patient was diagnosed BD after an immunology consultation. OS lens extraction was performed under explained prognosis.
 The vision improved minimally after the surgery to
counting fingers close to face, and remained stable for
2 years when he again presented in the emergency with
sudden onset painful vision loss OD. He had developed
phacotopic glaucoma, with complete anterior dislocation of
lens leading to IOP of 60 mmHg (Figure 1). He underwent
an urgent lens extraction OD, and corrected visual acuity
improved to counting fingers close to face. Three months
hence, condition is stable OU with stable vision, normal
IOP and quiescent uveitis.
The vision improved minimally after the surgery to
counting fingers close to face, and remained stable for
2 years when he again presented in the emergency with
sudden onset painful vision loss OD. He had developed
phacotopic glaucoma, with complete anterior dislocation of
lens leading to IOP of 60 mmHg (Figure 1). He underwent
an urgent lens extraction OD, and corrected visual acuity
improved to counting fingers close to face. Three months
hence, condition is stable OU with stable vision, normal
IOP and quiescent uveitis.
Pediatric BD are known to commonly present as panuveitis with retinal vasculitis, having poor visual prognoses and high odds of ocular complications like optic atrophy, especially in presence of HLA B5 positivity (1). While the diagnosis of BD was straightforward as per the International criteria (3), we could not identify any known cause of EL. EL in our case appears to be a complication of the ocular inflammation. Spontaneous lens subluxation is a known end result of long standing uveitis and has been described with Vogt Koyanagi Harada syndrome, sarcoidosis and pars planitis (4). Hence accumulation of end products of inff ammation in a closed compartment like the eye ball may result in zonular weakness, especially due to the proximity of the zonules and the zonular girdle to the uvea. In fact, late post-operative bag—IOL dislocations have also been seen in eyes having uveitis (5). Accumulation of inflammatory end products over the zonules and the lens capsule has been seen in cases of BD histo-pathologically too (6). EL, therefore, could have occurred due a combination of capsular shrinkage as well zonular dehiscence. Because of different genetics (3) and uncommon targets of inflammation (3,7), direct association between BD and EL is unlikely. Also the unsynchronized occurrence of ocular BD and EL in our case renders this association unlikely.
Hence, EL may occur as a complication of long standing panuveitis in cases of BD. The visual prognoses largely depend on functional status of the posterior segment.
A 20-year-old male presented to our clinic with severe vision loss since 10–12 years of age, along with history of recurrent redness and pain in early childhood that was managed with topical and oral steroids as per old documents. There were definite history and signs of multiple apthosis; oral as well as genital; along with positivity for HLA B5, but no significant family history or mental disability. The vision loss had become more severe in the past few years with present corrected visual acuity being hand motions close to face OU. OU subluxation of the lens was noted, OS having dense absorbed cataract with capsular fibrosis while OD had complicated posterior subcapsular cataract (Figure 1). There were also signs of previous panuveitis OU, with few old keratic precipitates in both the eyes accompanied by severe sclerosing mixed retinal vasculitis, maculopathy and optic atrophy (Figure 2). Intra ocular pressure (IOP) was normal OU. Serum Treponemal antibody tests were negative and urine examination was negative for amino aciduria. Marfan’s syndrome was ruled out with Echocardiography. The patient was diagnosed BD after an immunology consultation. OS lens extraction was performed under explained prognosis.
Figure 1 Clinical photographs of the anterior segment. (A) Subluxated cataractous lens OS. Note the anterior capsular shrinkage/dense plaque with remnants of posterior synechiae; (B) subluxated lens OD with complicated cataract; (C) anteriorly dislocated cataractous lens OD noted after follow-up of 2 years. Note the conjunctival congestion due to acute glaucoma.
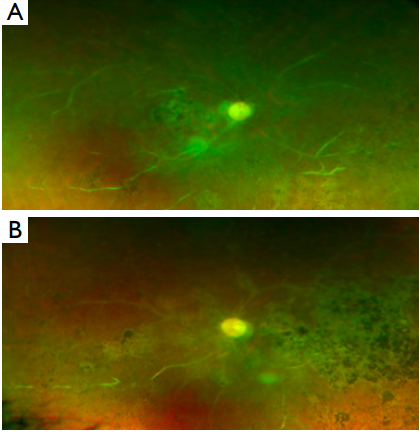
Figure 2 Ultra-wide fundus photograph OU depicting mixed vascular sclerosis, macular atrophy and optic atrophy. Pigmentary changes can also be seen throughout the fundus.
Pediatric BD are known to commonly present as panuveitis with retinal vasculitis, having poor visual prognoses and high odds of ocular complications like optic atrophy, especially in presence of HLA B5 positivity (1). While the diagnosis of BD was straightforward as per the International criteria (3), we could not identify any known cause of EL. EL in our case appears to be a complication of the ocular inflammation. Spontaneous lens subluxation is a known end result of long standing uveitis and has been described with Vogt Koyanagi Harada syndrome, sarcoidosis and pars planitis (4). Hence accumulation of end products of inff ammation in a closed compartment like the eye ball may result in zonular weakness, especially due to the proximity of the zonules and the zonular girdle to the uvea. In fact, late post-operative bag—IOL dislocations have also been seen in eyes having uveitis (5). Accumulation of inflammatory end products over the zonules and the lens capsule has been seen in cases of BD histo-pathologically too (6). EL, therefore, could have occurred due a combination of capsular shrinkage as well zonular dehiscence. Because of different genetics (3) and uncommon targets of inflammation (3,7), direct association between BD and EL is unlikely. Also the unsynchronized occurrence of ocular BD and EL in our case renders this association unlikely.
Hence, EL may occur as a complication of long standing panuveitis in cases of BD. The visual prognoses largely depend on functional status of the posterior segment.
基金
暂无基金信息
参考文献
1. Tugal-Tutkun I, Urgancioglu M. Childhood-onset uveitis in Behçet disease:a descriptive study of 36 cases. Am J Ophthalmol 2003;136:1114-9.
2. Hsu HY, Edelstein SL, Lind JT. Surgical management of non-traumatic pediatric ectopia lentis: A case series and review of the literature. Saudi J Ophthalmol 2012;26:315-21.
3. Ozen S. Pediatric onset Behçet disease. Curr Opin Rheumatol 2010;22:585-9.
4. Belfort R Jr, Nussenblatt RB, Lottemberg C, et al. Spontaneous lens subluxation in uveitis. Am J Ophthalmol 1990;110:714-6.
5. Steeples LR, Jones NP. Late in-the-bag intraocular lens dislocation in patients with uveitis. Br J Ophthalmol 2015;99:1206-10.
6. Goto M, Ujihara H, Ishii Y, et al. Immunohistological Investivation of the Conjunctiva, Lens Capsule and Iris in Behçet’s Disease. Invest Ophthalmol Vis Sci 2010;51:3787.
7. Bron AJ, Tripathi RC, Tripathi BJ. editors. Wolff ’s Anatomy of the Eye and Orbit. 8th edition. London: Chapman and Hall, 1997.