Ophthalmic complications related to dengue fever: a case report
阅读量:1365
DOI:doi: 10.3978/ j.issn.1000-4432.2016.09.09
发布日期:2024-12-02
作者:
Ruihong Ju ,Jinglin Zhang
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Dengue fever
ophthalmic complications
foveolitis
optical coherence tomography (OCT)
摘要
Two patients aged of 30 and 22 (female in cases 1, and male in case 2) both complained of
unilateral blurring of vision and scotoma within a week of being diagnosed with dengue fever. No other
abnormal findings were found in their anterior segment. Retinal examination revealed blurring of the optic
disc margin and several white spots in the posterior in both cases. Optical coherence tomography (OCT)
imagery revealed that the white spots were only located in the retinal outer layers. Macular cystic foveolitis
were also found in case 1 and diff used macular edema in case 2. In case 1, visual and retinal recovery were
seen to resolve spontaneously. In case 2, patient had complete visual recovery two months after onset of the
disease after being treated with steroids but central scotomata has continued to persist.
全文
Case presentation
Case 1
A 30-year-old woman, Han People, diagnosed with dengue fever by dengue polymerase chain reaction (PCR) test, presented with retrobulbar pain in both eyes two days after the onset of fever. Seven days after onset of fever, she had central scotoma, floaters and blurring of vision in the left eye which coincided with thrombocytopenia and leukopenia. She had experienced high myopia in both eyes since she was a teenager. Her best corrected visual acuity (BCVA) of both eyes was above 1.0. All symptoms and test results were normal in the right eye. Left eye BCVA was 0.3 and its introcular pressure was normal. No other abnormal findings were found in the anterior segment. Retinal examination revealed blurring of the optic disc margin and several white spots in the posterior retina which were only around the retinal capillaries (Figure 1A,B,C,D). Optical coherence tomography (OCT) imagery revealed that the white spots were only located in the retinal outer layers (Figure 1E,F), and also macular cystic foveolitis and breakage of the inner segment/ outer segment junction (IS/OS junction) (Figure 1E,G). Vitreous cells were also observed (Figure 1F,G). Central scotomata and floaters gradually decreased while platelets and leukocyte levels improved. Visual and retinal recovery were completely gained 20 days after the onset of disease without any treatment. However, the OCT imagery still showed a slight disruption of the IS/OS junction in the same place (Figure 1H).Case 2
A 22-year-old man, Han people, with diagnosis confirmed by detection of dengue-specific IgM antibodies (IgM enzyme-linked immunoassay), complained of bilateral central scotomata, floaters and blurring of vision after contracting dengue fever seven days prior. He also complained of high myopia in both eyes since he was a teenager. BCVA of both eyes were above 1.0 before the onset of dengue fever. The BCVA of both eyes were 0.4 and intraocular pressures were normal. There were no other abnormal findings in the anterior segment and vitreous cavity. Retinal examination revealed several white spots in the posterior retina, and blurring of the optic disc margin in both eyes. OCT imagery revealed diff use macular edema in the left eye. Fundus fluorecein angiography (FFA) showed staining of optic discs in both eyes. It also revealed a window defect due to retinal pigment epithelium (RPE) atrophy in the right eye and a leakage of venular and arteriolar over the entire posterior pole in the left eye. Central scotoma of the visual field was denoted as black squares. Visual recovery was completely gained two month after the onset of disease without any treatment. However, central scotomata has continued to persisted.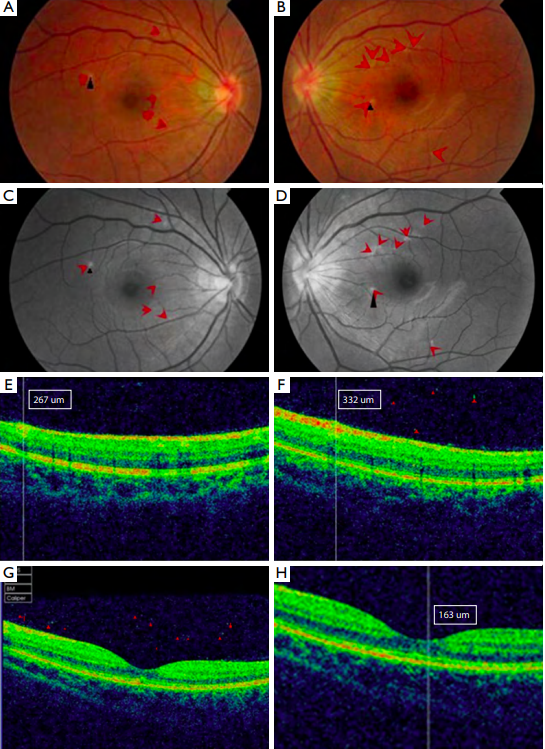
Discussion
Dengue fever, the most common mosquitoborne viral
disease in humans, is a multisystemic disease with known
complications(1), which includes blurring of vision,
scotoma, ocular pain, metamorphopsia, micropsia,
impairment of color vision and floaters. It usually occurs
within the first month after contracting dengue fever. The
main ocular findings have been found in both anterior
and posterior segments which include subconjunctival
hemorrhages, anterior uveitis, vitritis, macular and retina
hemorrhage, diffused retina edema, Roth’s spot, macular
yellow spots, and optic disc swelling(1). FFA showed
leakage in the optic disc and retinal vessels, macular
nonperfusion, and RPE defects, suggesting that the retina
and RPE were the primary sites of involvement. The
pathophysiological mechanism behind dengue infection
and ocular involvement is still unclear, but is speculated
to be related to an immune-mediated process(2,3). The
aggressive immune response may cause increased capillary
permeability, plasma leakage, and hemorrhagic diathesis.
This hemorrhage bleeding tendency can occur in both
the retina and choroid causing retina hemorrhage and
choroidal circulatory disorders. The outer retina layer is fed
by choroidal circulation making it vulnerable to ischemic
diseases.
In this study, both patients tested positive for dengue serology. It was noted that similar symptoms and retina changes occurred in both cases, which could be explained by the immune theory. The white spots were found in the retinal outer layers and only around the retinal capillaries. According to the immune-mediated process(2,3), the pathophysiological mechanism of these white spots may be explained by antigen-antibody complex deposit around venular and arteriolar because of the increased capillary permeability.
Both patients’ initial symptoms were also characteristic of multiple evanescent white dot syndrome (MEWDS): multiple yellow-white spots at the level of multiple layers of the retina, RPE, choriocapillaris, and the choroid. Jampol et al.(4)suggested that MEWDS was a specific type of autoimmune disease, which was usually a self-limiting condition with patients recovering and achieving a good visual acuity within several weeks. Choroidal circulation disturbance may also be involved. Therefore, it is doubtful that both disease have similar or same immune-mediated process.
In this study, both patients tested positive for dengue serology. It was noted that similar symptoms and retina changes occurred in both cases, which could be explained by the immune theory. The white spots were found in the retinal outer layers and only around the retinal capillaries. According to the immune-mediated process(2,3), the pathophysiological mechanism of these white spots may be explained by antigen-antibody complex deposit around venular and arteriolar because of the increased capillary permeability.
Both patients’ initial symptoms were also characteristic of multiple evanescent white dot syndrome (MEWDS): multiple yellow-white spots at the level of multiple layers of the retina, RPE, choriocapillaris, and the choroid. Jampol et al.(4)suggested that MEWDS was a specific type of autoimmune disease, which was usually a self-limiting condition with patients recovering and achieving a good visual acuity within several weeks. Choroidal circulation disturbance may also be involved. Therefore, it is doubtful that both disease have similar or same immune-mediated process.
Herbort et al.(5)reported tha t infl amma tor y conditions related to myopia were conditions involving the choriocapillaris. It could be hypothesized that fragility of the choriocapillaris due to particular anatomic changes caused by myopia, together with unknown immunogenetic factors, predispose myopic eyes to primary inflammatory choriocapillaropathies. In the study, both patients complained of high-myopia. It was speculated whether there was a connection between high-myopia and denguerelated ocular complications, which would need research.
The prognosis for ophthalmic complications is good with improved visual acuity and resolution of ocular signs in most patients without any treatment. While visual recovery usually corresponds with improving platelets levels, however, scotomata may persist for several weeks in some cases despite the resolution of ocular signs(1).
In conclusion, with the emergence of dengue fever, ophthalmologists should be aware and vigilant towards patients with ocular complaints. OCT, FFA and visual field testing are useful tools in the assessment diagnosis and follow-up of the extent and severity of this ocular disease.
基金
暂无基金信息
参考文献
1. Yip VC, Sanjay S, Koh YT. Ophthalmic complications of dengue Fever: a systematic review. Ophthalmol Ther 2012;1:2
2. Chan DP, Teoh SC, Tan CS, et al. Ophthalmic complications of dengue. Emerg Infect Dis 2006;12:285-9.
3. Su DH, Bacsal K, Chee SP, et al. Prevalence of dengue maculopathy in patients hospitalized for dengue fever. Ophthalmology 2007;114:1743-7.
4. Jampol LM, Becker KG. White spot syndromes of the retina: a hypothesis based on the common genetic hypothesis of autoimmune/inff ammatory disease. Am J Ophthalmol 2003;135:376-9.
5. Herbort CP, Papadia M, Neri P. Myopia and inff ammation. J Ophthalmic Vis Res 2011;6:270-83.
相关文章
甘雨虹;文峰;周孝来,A man with asymmetric bilateral choroidal melanocytosis: a case report and literature review丘蔚晴;张夏茵;赵兰琴;刘冬;温静怡;陈霞;王倩;李慧群;陈彦茹;韩彤;叶增纯;吴倩妮;林铎儒;肖辉;彭晖;林浩添,Retinal neurovascular characteristics for the diagnosis and staging of nondiabetic chronic kidney disease: a diagnostic study孟丽慧;于仟仪;杨景元;陈有信,Application of anterior scleral thickness measurement in different ocular conditions using anterior segment optical coherence tomography: a systemic review