The analysis of macular perimetry with octopus 900 in acute central serous chorioretinopathy
阅读量:1237
DOI:doi: 10.3978/j.issn.1000-4432.2016.08.01
发布日期:2024-12-01
作者:
Lin Yao ,Xuxia Meng ,Haiqing Ba
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Central serous chorioretinopathy (CSC)
macular perimetry (MP)
macular function
摘要
Background: To find the changes of macular perimetry (MP) and the correlations between MP and best
correct visual acuity (BCVA) in different phases of the acute central serous chorioretinopathy (CSC).
Methods: Twenty-one eyes with acute CSC and their fellow eyes were analysed retrospectively. MP at 2°, 4°
and BCVA in the active and resolved phase were collected and analyzed. The differences of these parameters
in CSC eyes and fellow eyes were analyzed. Spearman correlation was used for analysis of correlation
between MP and BCVA.
Results: From 29 eyes with CSC analysed 27eyes (93.10%) recovered to the previous VA. Compared with
the active phase, MP at 2°, 4° and BCVA were significantly improved in the resolved phase(P=0.000, 0.000,
0.000, respectively). MP at 2°, 4° and BCVA of CSC eyes were significantly poor compared with the fellow
eyes in the active phase (P=0.000, 0.000, 0.000, respectively). In the resolved phase there was no significant
difference between the CSC eyes and fellow eyes (P=0.339, 0.141, 0.161, respectively). BCVA was shown to
significantly correlate with MP at 2° in the active phase (ρ=–0.630, P<0.001).
Conclusions: The acute CSC often had a good prognosis both in BCVA and MP. MP can provide an
additional objective parameter to evaluate the retinal function changes at macula of acute CSC.
全文
Introduction
The central serous chorioretinopathy (CSC) is a
disorder confined to the macula, characterized by serous
neurosensory retina and/or retinal pigment epithelium
(RPE) detachment due to choroidal hyperpermeability and
focal RPE defect. Clinically, CSC is classified as acute and
chronic. Classic CSC occurs in an acute form, characterized
by acute retinal detachment within macula, with mild
to moderate blurred central vision, metamorphopsia,
dyschromatopsia, shallow relative scotoma, mild diopter
changes, minimal focal RPE damage and leakage by
fluorescein angiography (FA). Acute CSC generally resolves
spontaneously within months, and observation is advisable
following the initial diagnosis of acute CSC in the majority
of patients (1-3). Chronic CSC is defined as persistent
central retinal detachment for 3 to 6 months, may cause
permanent visual loss. FA shows extensive RPE damage
and diffuse leakage (1). Verteporfin photodynamic therapy
(PDT) and focal laser photocoagulation are the main
treatment therapies for chronic CSC currently (4-6).
Although the visual acuity is relatively good in most of the acute CSC patients, macular functional damage is observed in some focal areas (7). Therefore, the mild blurred vision does not always consistent with the severity of the disease. Recently, macular perimetry (MP) is introduced automatic fundus perimeter, which has been shown to be eff ective in assessing the macular function in some macular pathologies (4,8,9). In some chronic and resolved CSC studies, MP has been used to evaluate the macular retina function (5,8,10,11). However, in acute CSC, the change of MP in active and resolved phase has rarely been mentioned.
The aim of this study was to find the change of MP and the correlation between MP and best correct visual acuity (BCVA) in the diff erent phase of acute CSC.
Although the visual acuity is relatively good in most of the acute CSC patients, macular functional damage is observed in some focal areas (7). Therefore, the mild blurred vision does not always consistent with the severity of the disease. Recently, macular perimetry (MP) is introduced automatic fundus perimeter, which has been shown to be eff ective in assessing the macular function in some macular pathologies (4,8,9). In some chronic and resolved CSC studies, MP has been used to evaluate the macular retina function (5,8,10,11). However, in acute CSC, the change of MP in active and resolved phase has rarely been mentioned.
The aim of this study was to find the change of MP and the correlation between MP and best correct visual acuity (BCVA) in the diff erent phase of acute CSC.
Methods
A retrospective chart review was performed of consecutive
patients with acute CSC in our hospital between May
01 2012 and April 30 2013. The study was approved by
the Research Ethics Committee of Affiliated Hospital of
Qingdao University (approval ID: 2012-011). And the
records of the patients were anonymized and de-identiff ed
prior to analysis.
Acute CSC was diagnosed as the presence of serous neurosensory retina detachment involving the macula, conff rmed by macular optical coherence topography (OCT) and the leakage at the level of the RPE on FA, and self revolved in 6 months. Active phase was defined as serous neurosensory retina detachment involving the macula. Resolved phase was deff ned by the absence of detachment at the time of OCT measurement.
In addition to OCT and FA, patients underwent BCVA measurements, MP, automated refraction, noncontact tomometer, slit-lamp biomicroscope, and indirect ophthalmoscopy at the first visit in the active and resolved phase. Additional data were recorded for each patient included sex and age.
We compared the BCVA and MP in the active and resolved phase of the CSC eyes. We also compared the BCVA and MP in CSC eyes and fellow eyes, and analyzed the correlation between them in diff erent phase.
MP was performed with the octopus 900 perimetry (Haag-Streit International, Koeniz, Switzerland). Threshold fundus perimetry was performed on the central 2° and 4° in diameter of the retina. Golemann III size white-cross stimuli and a 4- to 2- to 1-dB staircase threshold strategy were used. White on white static perimetry was performed with a background luminance of 4 asb with a pericentral diamond ff xation target, and a stimulus duration of 200 ms. And 17 stimulus points (8 ring-shaped points and 1 center point for the central 2° and 8 ring-shaped points for the center 2°–4°) covering the central 4° in diameter of the retina were applied. The mean macular sensitivities for the central 2° and 4° were then calculated.
Comparisons of the parameters between active and resolved phase of CSC eyes and normal fellow eyes were obtained using paired t-test for independent sample. Moreover, Spearman correlation analysis was performed to MP and BCVA. Statistical analysis was performed using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA). A P value less than 0.05 was considered statistically significant.
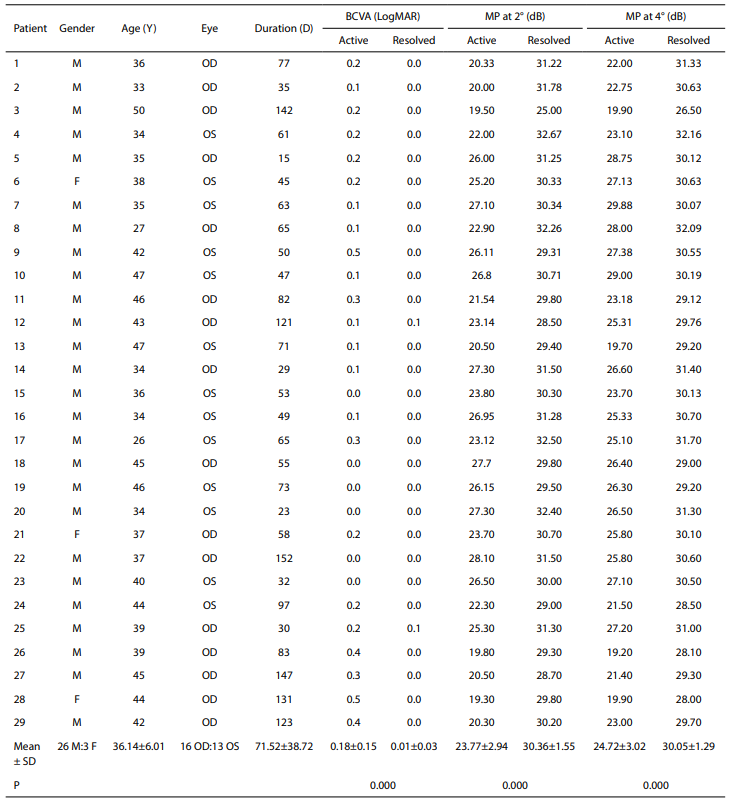
CSC, central serous chorioretinopathy; BCVA, best corrected visual acuity; MP, macular perimetry; F, female; M, male; Y, year; D, day; SD, standard deviation; LogMAR, logarithm of the minimum angle of resolution.
In our study, we also analyzed the correlation between MP at 2°, 4° and BCVA in active and resolved phase. In the active phase, we found BCVA was significantly correlated with MP at 2°, which represents the central fovea, but not MP at 4°, which involves the whole macula. Probably because the central fovea is more affected or tends to present the higher detachement. This may be because the damage of CSC was mainly at the fovea. And MP at 2° could represent the function of the fovea more exactly. In another study, BCVA was shown to correlate with MP at 2° and 4° in the resolved CSC (12). Nevertheless, in the resolved phase, we found there was no significant correlation between them. Most of our patients (93.10%) resolved to normal BCVA in the resolved phase. Meanwhile, neither MP at 2° nor 4° had significant difference between CSC eyes and the normal fellow eyes. This may be why there was no correlation between MP and BCVA in the resolved phase in our study.
Acute CSC was diagnosed as the presence of serous neurosensory retina detachment involving the macula, conff rmed by macular optical coherence topography (OCT) and the leakage at the level of the RPE on FA, and self revolved in 6 months. Active phase was defined as serous neurosensory retina detachment involving the macula. Resolved phase was deff ned by the absence of detachment at the time of OCT measurement.
In addition to OCT and FA, patients underwent BCVA measurements, MP, automated refraction, noncontact tomometer, slit-lamp biomicroscope, and indirect ophthalmoscopy at the first visit in the active and resolved phase. Additional data were recorded for each patient included sex and age.
We compared the BCVA and MP in the active and resolved phase of the CSC eyes. We also compared the BCVA and MP in CSC eyes and fellow eyes, and analyzed the correlation between them in diff erent phase.
MP was performed with the octopus 900 perimetry (Haag-Streit International, Koeniz, Switzerland). Threshold fundus perimetry was performed on the central 2° and 4° in diameter of the retina. Golemann III size white-cross stimuli and a 4- to 2- to 1-dB staircase threshold strategy were used. White on white static perimetry was performed with a background luminance of 4 asb with a pericentral diamond ff xation target, and a stimulus duration of 200 ms. And 17 stimulus points (8 ring-shaped points and 1 center point for the central 2° and 8 ring-shaped points for the center 2°–4°) covering the central 4° in diameter of the retina were applied. The mean macular sensitivities for the central 2° and 4° were then calculated.
Comparisons of the parameters between active and resolved phase of CSC eyes and normal fellow eyes were obtained using paired t-test for independent sample. Moreover, Spearman correlation analysis was performed to MP and BCVA. Statistical analysis was performed using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA). A P value less than 0.05 was considered statistically significant.
Results
Baseline characteristics
The baseline demographic data are shown in Table 1. Fiftyeight eyes from 29 patients were analyzed. The average patient age was 36.14±6.01 (range, 26–50) years. Twentysix (89.66%) were male. The number of right and left CSC eyes was 16 and 13, respectively. The mean duration was 71.52±38.72 (range, 15–152) days.Table 1 Clinical characteristics of acute CSC patients in active and resolved phase
CSC, central serous chorioretinopathy; BCVA, best corrected visual acuity; MP, macular perimetry; F, female; M, male; Y, year; D, day; SD, standard deviation; LogMAR, logarithm of the minimum angle of resolution.
BCVA and MP
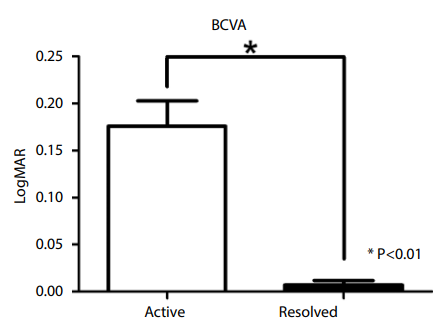
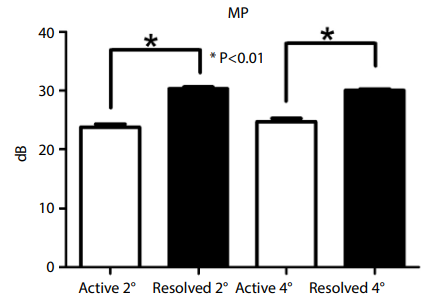
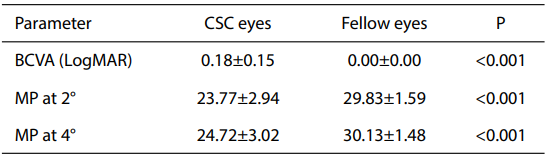
About the BCVA, 27 (93.10%) CSC eyes recovered in the resolved phase. Twenty-two (75.86%) CSC eyes resolved in 3 months, and 7 (24.14%) CSC eyes resolved between 3 to 6 months. Compared with the active phase, MP at 2°, 4° and BCVA were significantly improved in the resolved phase (P<0.001) (Table 1, Figures 1,2). In the active phase, MP at 2°, 4° and BCVA of CSC eyes were signiff cantly poor compared with the fellow eyes (P<0.001) (Table 2). However, in the resolved phase there were no significantly difference between the CSC eyes and fellow eyes (P=0.339, 0.141, 0.161, respectively) (Table 3).Figure 1 Best correct visual acuity (BCVA) of the active and resolved phases.
Figure 2 Macular perimetry (MP) of the active and resolved phases.
Table 2 BCVA and MP in active phase
CSC, central serous chorioretinopathy; BCVA, best corrected
visual acuity; MP, macular perimetry; CSC, central serous
chorioretinopathy; LogMAR, logarithm of the minimum angle of
resolution.
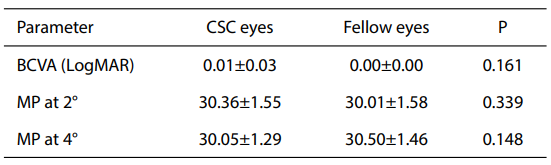
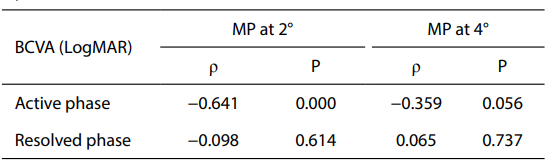
Table 3 BCVA and MP in resolved phase
BCVA, best corrected visual acuity; MP, macular perimetry;
CSC, central serous chorioretinopathy; LogMAR, logarithm of
the minimum angle of resolution.
BCVA was shown to significantly correlate with MP
at 2° in the active phase (ρ=–0.630, P<0.001). BCVA was
consistent with macular sensitivities at 2°. However, there
was not signiff cant correlation between them in the resolved
phase (ρ=–0.098, P=0.614). Also, no significant correlation
was seen between BCVA and MP at 4° in both active and
resolved phase (ρ=–0.359, P=0.056; ρ=–0.065, P=0.737;
respectively) (Table 4). Table 4 Correlation between BCVA and MP in active and resolved phase
BCVA, best corrected visual acuity; MP, macular perimetry;
LogMAR, logarithm of the minimum angle of resolution.
Discussion
The study analyzed the BCVA and MP of acute CSC in different phases, and evaluated the possible correlation
between BCVA and MP.
CSC is considered a self-limiting condition with good prognosis, and therefore, expectant management including observation and change in lifestyle is considered first-line. Most of the previous studies focus on the chronic CSC and resolved CSC (10-13). In this study we focus on the acute CSC, especially in the active phase and the early stage of the resolved phase.
Some previous studies took 3 months as the deadline to divide the acute and chronic CSC (14,15). However, in this study we took 6 months as the deadline of the acute CSC as other studies (1,2,8). In our study, 22 (75.86%) of the 29 acute CSC patients resolved in 3 months, and other 7 (24.14%) patients resolved in 6 months without any treatment. So we think 6 months may be more appropriate to distinct the acute and chronic CSC.
BCVA is the standard way to measure visual performance, however it does not describe the full extent of the functional impact on visual performance in the acute CSC patients. MP is one of the functional evaluation techniques, which can evaluate the retinal sensitivity and central retinal field function. BCVA combined with MP was considered to be more informative to explain the visual function of the CSC patients (13,16,17). In the present study, we performed MP to objectively evaluate the changes in macular function of the CSC in the active and resolved phase. Compared with the active phase, both MP at 2°, 4° and BCVA were significantly improved in the resolved phase. However, there were no signiff cant diff erence between CSC eyes and fellow eyes in the resolved phase. This result was different to other previous studies of the resolved CSC. Chung et al. found MP was significantly decreased in the points with loss of the ellipsoid portion of the inner segments (EPIS) in the resolved CSC eyes (10). In another study, they also found MP at the fovea had a significant association with the EPIS defect (12). This may be because our patients were acute CSC and resolves spontaneously within months. Usually, these patients had a better prognosis. Our study demonstrated that the impaction of CSC on the BCVA and MP of these patients was not obvious in the resolved phase. Thus, observation may be the ff rst choice for these patients. After all, the treatment with laser and PDT has risks including choroidal ischemia, RPE atrophy and iatrogenic CNV (18-21).
CSC is considered a self-limiting condition with good prognosis, and therefore, expectant management including observation and change in lifestyle is considered first-line. Most of the previous studies focus on the chronic CSC and resolved CSC (10-13). In this study we focus on the acute CSC, especially in the active phase and the early stage of the resolved phase.
Some previous studies took 3 months as the deadline to divide the acute and chronic CSC (14,15). However, in this study we took 6 months as the deadline of the acute CSC as other studies (1,2,8). In our study, 22 (75.86%) of the 29 acute CSC patients resolved in 3 months, and other 7 (24.14%) patients resolved in 6 months without any treatment. So we think 6 months may be more appropriate to distinct the acute and chronic CSC.
BCVA is the standard way to measure visual performance, however it does not describe the full extent of the functional impact on visual performance in the acute CSC patients. MP is one of the functional evaluation techniques, which can evaluate the retinal sensitivity and central retinal field function. BCVA combined with MP was considered to be more informative to explain the visual function of the CSC patients (13,16,17). In the present study, we performed MP to objectively evaluate the changes in macular function of the CSC in the active and resolved phase. Compared with the active phase, both MP at 2°, 4° and BCVA were significantly improved in the resolved phase. However, there were no signiff cant diff erence between CSC eyes and fellow eyes in the resolved phase. This result was different to other previous studies of the resolved CSC. Chung et al. found MP was significantly decreased in the points with loss of the ellipsoid portion of the inner segments (EPIS) in the resolved CSC eyes (10). In another study, they also found MP at the fovea had a significant association with the EPIS defect (12). This may be because our patients were acute CSC and resolves spontaneously within months. Usually, these patients had a better prognosis. Our study demonstrated that the impaction of CSC on the BCVA and MP of these patients was not obvious in the resolved phase. Thus, observation may be the ff rst choice for these patients. After all, the treatment with laser and PDT has risks including choroidal ischemia, RPE atrophy and iatrogenic CNV (18-21).
In our study, we also analyzed the correlation between MP at 2°, 4° and BCVA in active and resolved phase. In the active phase, we found BCVA was significantly correlated with MP at 2°, which represents the central fovea, but not MP at 4°, which involves the whole macula. Probably because the central fovea is more affected or tends to present the higher detachement. This may be because the damage of CSC was mainly at the fovea. And MP at 2° could represent the function of the fovea more exactly. In another study, BCVA was shown to correlate with MP at 2° and 4° in the resolved CSC (12). Nevertheless, in the resolved phase, we found there was no significant correlation between them. Most of our patients (93.10%) resolved to normal BCVA in the resolved phase. Meanwhile, neither MP at 2° nor 4° had significant difference between CSC eyes and the normal fellow eyes. This may be why there was no correlation between MP and BCVA in the resolved phase in our study.
基金
暂无基金信息
参考文献
1. Wang M, Munch IC, Hasler PW, et al. Central serous chorioretinopathy. Acta Ophthalmol 2008;86:126-45.
2. Eandi CM, Ober M, Iranmanesh R, et al. Acute central serous chorioretinopathy and fundus autoff uorescence. Retina 2005;25:989-93.
3. Fine HF, Ober MD, Hariprasad SM. Current concepts in managing central serous chorioretinopathy. Ophthalmic Surg Lasers Imaging Retina 2014;45:9-13.
4. Senturk F, Karacorlu M, Ozdemir H, et al. Microperimetric changes after photodynamic therapy for central serous chorioretinopathy. Am J Ophthalmol 2011;151:303-9.e1
5. Fujita K, Shinoda K, Matsumoto CS, et al. Microperimetric evaluation of chronic central serous chorioretinopathy after half-dose photodynamic therapy. Clin Ophthalmol 2012;6:1681-7.
6. Kim JY, Park HS, Kim SY. Short-term efficacy of subthreshold micropulse yellow laser (577-nm) photocoagulation for chronic central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol 2015;253:2129-35.
7. Ojima Y, Tsujikawa A, Hangai M, et al. Retinal sensitivity measured with the micro perimeter 1 after resolution of central serous chorioretinopathy. Am J Ophthalmol
2008;146:77-84.
8. Eandi CM, Piccolino FC, Alovisi C, et al. Correlation between fundus autoff uorescence and central visual function in chronic central serous chorioretinopathy. Am J Ophthalmol 2015;159:652-8.
9. Lim JW, Kang SW, Kim YT, et al. Comparative study of patients with central serous chorioretinopathy undergoing focal laser photocoagulation or photodynamic therapy. Br
J Ophthalmol 2011;95:514-7.
10. Chung HW, Yun CM, Kim JT, et al. Retinal sensitivity assessed by microperimetry and corresponding retinal structure and thickness in resolved central serous chorioretinopathy. Eye (Lond) 2014;28:1223-30.
11. Oh J, Kim SW, Kwon SS, et al. Correlation of fundus autoff uorescence gray values with vision and microperimetry in resolved central serous chorioretinopathy. Invest Ophthalmol Vis Sci 2012;53:179-84.
12. Kim SW, Oh J, Huh K. Correlations among various functional and morphological tests in resolved central serous chorioretinopathy. Br J Ophthalmol 2012;96:350-5.
13. Ozdemir H, Karacorlu SA, Senturk F, et al. Assessment of macular function by microperimetry in unilateral resolved central serous chorioretinopathy. Eye (Lond) 2008;22:204-8.
14. Liew G, Quin G, Gillies M, et al. Central serous chorioretinopathy: a review of epidemiology and pathophysiology. Clin Experiment Ophthalmol 2013;41:201-14.
15. Roisman L, Ribeiro JC, Fechine FV, et al. Does microperimetry have a prognostic value in central serous chorioretinopathy? Retina 2014;34:713-8.
16. Ozdemir H, Senturk F, Karacorlu M, et al. Macular sensitivity in eyes with central serous chorioretinopathy. Eur J Ophthalmol 2008;18:799-804.
17. Schmidt-Erfurth UM, Elsner H, Terai N, et al. Eff ects of verteporff n therapy on central visual ff eld function. Ophthalmology 2004;111:931-9.
18. Koytak A, Erol K, Coskun E, et al. Fluorescein angiography-guided photodynamic therapy with half-dose verteporff n for chronic central serous chorioretinopathy. Retina 2010;30:1698-703.
19. Lai TY, Chan WM, Li H, et al. Safety enhanced photodynamic therapy with half dose verteporff n for chronic central serous chorioretinopathy: a short term pilot study. Br J Ophthalmol 2006;90:869-74.
20. Reibaldi M, Cardascia N, Longo A, et al. Standard-ff uence versus low-ff uence photodynamic therapy in chronic central serous chorioretinopathy: a nonrandomized clinical trial. Am J Ophthalmol 2010;149:307-315.e2.
21. Williams MA, Mulholland C, Silvestri G. Photodynamic therapy for central serous chorioretinopathy using a reduced dose of verteporff n. Can J Ophthalmol 2008;43:123.
相关文章
Sailaja Bondalapati;Avinash Pathengay;Jay Chhablani,External drainage for exudative retinal detachment secondary to central serous chorioretinopathyZi Ye;Zhaohui Li;Shouzhi He;Bing Chen;Xiaojuan Xing;Chunyan Ren,Outcomes of Coaxial Micro-incision Phacoemulsification in Nanophthalmic Eyes: Report of Retrospective Case SeriesJinglin Zhang;Yonghao Li;Xiujuan Zhao;Yu Cai;Xiling Yu;Lin Lu,Relationship between full-thickness macular hole and retinal break/lattice degeneration