Relationship between full-thickness macular hole and retinal break/lattice degeneration
阅读量:1704
DOI:doi: 10.3978/j.issn.1000-4432.2015.11.02
发布日期:2025-01-01
作者:
Jinglin Zhang ,Yonghao Li ,Xiujuan Zhao ,Yu Cai ,Xiling Yu ,Lin Lu
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Macular hole (MH)
retinal break (RB)
lattice degeneration
optical coherence tomography (OCT)
vitreous retinopathy
摘要
Background: The purpose is to investigate the relationship between full-thickness macular hole (MH) and
retinal break (RB) and/or lattice degeneration.
Methods: Patients diagnosed as full-thickness MH and referred to Dr. Lin Lu from January 2009 to
December 2013 were evaluated. All patients underwent general ophthalmologic examinations, fundus
examination and optical coherence tomography (OCT). The RB and/or lattice degeneration were recorded.
Results: Totally 183 eyes of 167 patients were included. The sex ratio of men to women was 1:2.88. A
total of 17 eyes were pseudophakic and 166 eyes were phakic. RB and/or lattice degeneration were found
in 62 eyes (33.88%). The prevalence of RB and/or lattice degeneration was similar between men and
women (P=0.344>0.05). There was no statistical diff erence between the pseudophakic eyes and phakic eyes
(P=0.138>0.05). All of the RB and/or lattice degeneration were located near or anterior to the equator. The
inferior quadrants and the vertical meridian were aff ected more often than the superior quadrants and the
horizontal meridian.
Conclusions: We identified a high incidence of RB/lattice degeneration in cases of full-thickness MH.
Carefully examination of the peripheral retina and prophylactic treatment of RB and/or lattice degeneration
are critical.
全文
Introduction
The pathogenesis of full-thickness macular hole (MH)
is not clearly understood but is believed to involve
anteroposterior traction and/or tangential traction exerted
by the posterior vitreous cortex at the fovea(1). Retinal
break (RB) and lattice degeneration are one of the most
important abnormalities of vitreous and vitreoretinal
interface. To figure out the relationship between the fullthickness
MH and RB/lattice degeneration may contribute
to the understanding of their pathogenesis. We conducted
a prospective observational case series to investigate the
relationship between full-thickness MH and RB/lattice
degeneration.
OCT had disclosed a significant progression of posterior vitreous detachment after phacoemulsification(26). Even so, there is no evidence that RB/lattice degeneration deteriorates after phacoemulsification. In our study, the prevalence of RB/lattice degeneration in the MH cases were similar between the pseudophakic and phakic eyes. Interestingly, most of the full-thickness MH cases were phakic. The onset age of MH is relatively young might be the reason.
In conclusion, the prevalence of RB/lattice degeneration is high in full-thickness MH. Preoperative and intraoperative detection and treatment of RB/lattice degeneration are critical.
Methods
This is a prospective observational case series study
conducted according to the tenets of Declaration of
Helsinki. All patients gave informed consent to being imaged and for the collected data to be used for publication.
The Zhongshan Ophthalmic Center Ethics Committee did
not require for this study to undergo Internal Review Board
(IRB) approval as all the tests carried out were part of the
routine care of patients.
This study included patients who were diagnosed as fullthickness MH and referred to Dr. Lin Lu from January 2009 to December 2013 at the Zhongshan Ophthalmic Center. Patients suffering from MH secondary to uveitis, trauma, and high myopia or associated with a simultaneous retinal detachment (RD) were excluded. All the patients received a general ophthalmologic examination. The status of macular was confirmed by optical coherence tomography (OCT). MH were graded using the Gass classification(2). The fundus was carefully inspected by a three-minor Goldmann lens with a dilated pupil. The RB and/or lattice degeneration were recorded.
Numerical computations were per formed using a spreadsheet package (Excel 2010; Microsoft, Redmond, WA, USA). Statistical comparison of categorical findings was performed using the Chi-square test. Statistical signifi cance was set as P<0.05.
This study included patients who were diagnosed as fullthickness MH and referred to Dr. Lin Lu from January 2009 to December 2013 at the Zhongshan Ophthalmic Center. Patients suffering from MH secondary to uveitis, trauma, and high myopia or associated with a simultaneous retinal detachment (RD) were excluded. All the patients received a general ophthalmologic examination. The status of macular was confirmed by optical coherence tomography (OCT). MH were graded using the Gass classification(2). The fundus was carefully inspected by a three-minor Goldmann lens with a dilated pupil. The RB and/or lattice degeneration were recorded.
Numerical computations were per formed using a spreadsheet package (Excel 2010; Microsoft, Redmond, WA, USA). Statistical comparison of categorical findings was performed using the Chi-square test. Statistical signifi cance was set as P<0.05.
Results
In all, 183 eyes of 167 patients fulfilled the inclusion and
exclusion criteria. A total of 124 patients (74.25%) were
women. The sex ratio of men to women was 1:2.88. And
the 16 bilateral MH cases were all women. The mean age
of patients at presentation was 66.02±7.30 (range, 54 to
79) years. The mean duration of patients’ symptoms was
11.46±6.66 (range, 1 to 24) months.
Mean spherical equivalent refractive error was –1.17± 1.55 (range, –4.00 to 1.50) diopters. The mean intraocular pressure was 15.87±3.28 (range, 10 to 24) mmHg. Seventeen eyes (9.29%) were pseudophakic and the remaining 166 eyes (90.71%) were phakic. MH were most commonly graded as stage 3, followed by stage 4 and stage 2 (Table 1).
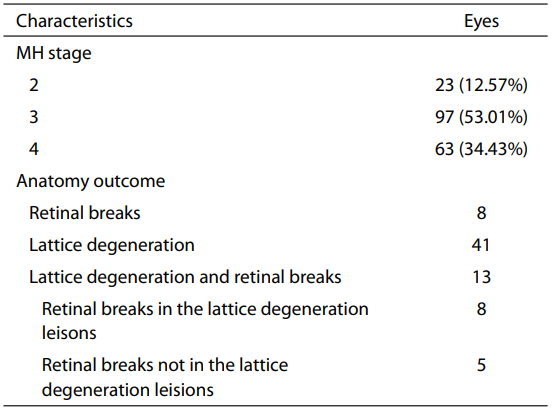 RB and/or lattice degeneration were detected in 62 eyes
(33.88%). Three of them had the history of prophylactic
laser photocoagulation. The lattice degeneration seems to
be more common than RB (Table 1). Most of the RB were
atrophic holes and only one of them was horseshoe-shaped
tear. The prevalence of RB and/or lattice degeneration was
similar (P=0.344>0.05) between men (12/43, 27.91%) and
women (50/140, 35.71%). Lattice degenerations were found
in three eyes of pseudophakic eyes. There was no statistical
difference between the pseudophakic eyes and phakic
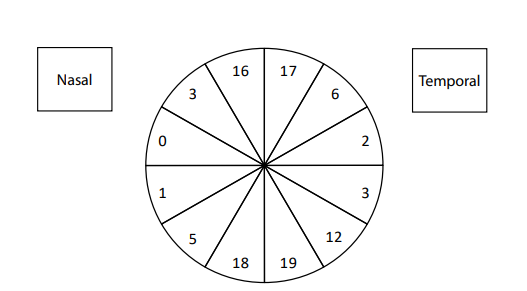
eyes (P=0.138>0.05). All of the RB/lattice degeneration
was located near or anterior to the equator. The inferior
quadrants and the vertical meridian were affected more
often than the superior quadrants and the horizontal
meridian (Figure 1).
RB and/or lattice degeneration were detected in 62 eyes
(33.88%). Three of them had the history of prophylactic
laser photocoagulation. The lattice degeneration seems to
be more common than RB (Table 1). Most of the RB were
atrophic holes and only one of them was horseshoe-shaped
tear. The prevalence of RB and/or lattice degeneration was
similar (P=0.344>0.05) between men (12/43, 27.91%) and
women (50/140, 35.71%). Lattice degenerations were found
in three eyes of pseudophakic eyes. There was no statistical
difference between the pseudophakic eyes and phakic
eyes (P=0.138>0.05). All of the RB/lattice degeneration
was located near or anterior to the equator. The inferior
quadrants and the vertical meridian were affected more
often than the superior quadrants and the horizontal
meridian (Figure 1).
Mean spherical equivalent refractive error was –1.17± 1.55 (range, –4.00 to 1.50) diopters. The mean intraocular pressure was 15.87±3.28 (range, 10 to 24) mmHg. Seventeen eyes (9.29%) were pseudophakic and the remaining 166 eyes (90.71%) were phakic. MH were most commonly graded as stage 3, followed by stage 4 and stage 2 (Table 1).
Table 1 Macular hole (MH) staging and anatomic outcome
Figure 1 Relative distribution of retina break (RB)/lattice
degeneration.
This figure showed the relative distribution of RB/
lattice degeneration. The lesions were somewhat more prevalent in
the inferior hemisphere (58/102, 56.87%). The vertical meridian
was aff ected more often than the horizontal meridian (70 vs. 6).Discussion
No previous study on the relationship between RB/lattice
degeneration and MH has been reported. Few studies
mentioned it indirectly and had a few limitations.
Guillaubey et al.(3) retrospectively analyzed 272 idiopathic
MH surgery cases. Only the cases of RB were recorded
and the lattice degenerations were not included. No RD occurred in patients presenting with an intraoperative
(14 eyes) or preoperative (21 eyes) successfully treated RB.
They didn’t mention the RB found during the procedure
was iatrogenic or not. If the RB found during the procedure
were already exist, the RB rate (12.87%) in their cases is
similar with ours cases (21/183=11.48%). In another study
by Hwang et al.(4), 235 MH surgery cases were reviewed.
Only eight eyes (3.40%) preexisted RB and/or lattice
degeneration before the surgery received intraoperative
endolaser photocoagulation. They only concerned about
the cases which had been treated during the operation and
didn’t present the status before the surgery. That’s why the
RB and/or lattice degeneration rate seems so low in their
series.
The prevalence of lattice degeneration of the retina ranges from 6% to 10.7% in the general populations(5-7). In the fellow eye of patients with RD the prevalence is estimated to be 35%(8). This study identified that RB and/or lattice degeneration were involved in almost one third of the full-thickness MH cases. It revealed MH and RB/lattice degeneration might have some pathogenic relationship.
Generally the attachment of the vitreous to the retina is greatest at those sites where the ILM of the retina is the thinnest. These sites include the vitreous base, the major retinal vessels, the optic nerve head, the 1,500-μm-diameter rim surrounding the fovea, and the 500-μm-diameter foveola. Forces generated by movement of the vitreous and the premacular bursa as the eye moves may also play a role in the pathogenesis of posterior vitreous detachment, MH and RB(9). This theory might explain why the RB and/or lattice degenerations found in our cases were located near or anterior to the equator. The RB/lattice degeneration was involved in the inferior temporal quadrant most often in our cases. A total of 68.63% of the lesions were found between the clock hours of 11 to 1 above, or between 5 and 7 below. These findings are similar to previously reported outcomes(5-7). The movement of the eyeball contributes to distribution of the lesions.
Not only the anatomic factors were involved but also
the genetic factors may play important roles. Pathogenic
features of lattice degeneration of retina include liquefaction
of the adjacent vitreous humor, absence of vitreoretinal
attachments, absence of the internal limiting membrane
(ILM) over the lesions, and vitreous condensation with
a firm vitreoretinal attachment at the lesion margins.
Pathogenesis may be due to a developmental abnormality
involving the ILM of the retina (10). It has been
demonstrated the presence of the α3 (IV) -α5 (IV) collagen
chains in the normal ILM as well as the RPE basement
membrane of Bruch’s membrane(11). Alport syndrome
is an inherited disease and characterized by renal failure,
hearing loss, lenticonus, and retinopathy(12). Mutations
in the COL4A3, -4 and -5 genes in Alport syndrome(13,14) result in the loss of α3 (IV) -α5 (IV ) collagen
network from affected basement membranes(15) and the
subsequent development of thinning or lamellation(16-18).
Vitreoretinal degeneration is complicated by RD in Alport
syndrome. Savige et al.(11) demonstrated the retinopathy
principally affected the ILM/nerve fiber layer (NFL). A
thinned ILM may be more susceptible to tractional forces
from the vitreous, interfere with the transport of nutrients,
or impair the clearance of waste products. Therefore
MH associated with Alport syndrome are rare, but they
are typically larger than those found in other conditions(19-23). What’s more, Smiddy and Flynn demonstrated
the importance of the role of degeneration of the inner
retinal layers in the formation of MH(24). Meguro
et al.(25) discovered COL4A4 on chromosome 2q36.3
was strongly associated with lattice degeneration of the
retina susceptibility. The variants in the COL4A4 gene may
contribute to the development of lattice degeneration of the
retina. We speculated that aberrations in COL4A4 may be
involved in cases of full-thickness MH. The prevalence of lattice degeneration of the retina ranges from 6% to 10.7% in the general populations(5-7). In the fellow eye of patients with RD the prevalence is estimated to be 35%(8). This study identified that RB and/or lattice degeneration were involved in almost one third of the full-thickness MH cases. It revealed MH and RB/lattice degeneration might have some pathogenic relationship.
Generally the attachment of the vitreous to the retina is greatest at those sites where the ILM of the retina is the thinnest. These sites include the vitreous base, the major retinal vessels, the optic nerve head, the 1,500-μm-diameter rim surrounding the fovea, and the 500-μm-diameter foveola. Forces generated by movement of the vitreous and the premacular bursa as the eye moves may also play a role in the pathogenesis of posterior vitreous detachment, MH and RB(9). This theory might explain why the RB and/or lattice degenerations found in our cases were located near or anterior to the equator. The RB/lattice degeneration was involved in the inferior temporal quadrant most often in our cases. A total of 68.63% of the lesions were found between the clock hours of 11 to 1 above, or between 5 and 7 below. These findings are similar to previously reported outcomes(5-7). The movement of the eyeball contributes to distribution of the lesions.
OCT had disclosed a significant progression of posterior vitreous detachment after phacoemulsification(26). Even so, there is no evidence that RB/lattice degeneration deteriorates after phacoemulsification. In our study, the prevalence of RB/lattice degeneration in the MH cases were similar between the pseudophakic and phakic eyes. Interestingly, most of the full-thickness MH cases were phakic. The onset age of MH is relatively young might be the reason.
In conclusion, the prevalence of RB/lattice degeneration is high in full-thickness MH. Preoperative and intraoperative detection and treatment of RB/lattice degeneration are critical.
基金
1. This article is supported by National Nature Science Foundation of China (NO.81170863).
参考文献
1. Bainbridge J, Herbert E, Gregor Z. Macular holes: vitreoretinal relationships and surgical approaches. Eye (Lond) 2008;22:1301-9.
2. Gass JD. Reappraisal of biomicroscopic classifi cation of stages of development of a macular hole. Am J Ophthalmol 1995;119:752-9.
3. Guillaubey A, Malvitte L, Lafontaine PO, et al. Incidence of retinal detachment after macular surgery: a retrospective study of 634 cases. Br J Ophthalmol 2007;91:1327-30.
4. Hwang J, Escariao P, Iranmanesh R, et al. Outcomes of macular hole surgery in patients treated intraoperatively for retinal breaks and/or lattice degeneration. Retina 2007;27:1243-8.
5. Straatsma BR, Zeegen PD, Foos RY, et al. XXX Edward Jackson Memorial Lecture. Lattice degeneration of the retina. Trans Am Acad Ophthalmol Otolaryngol 1974;78:OP87-113.
6. Byer NE. Clinical study of lattice degeneration of the retina. Trans Am Acad Ophthalmol Otolaryngol 1965;69:1065-81.
7. Byer NE. Lattice degeneration of the retina. Surv Ophthalmol 1979;23:213-48.
8. Madjarov B, Hilton GF, Brinton DA, et al. A new classification of the retinoschises. Retina 1995;15:282-5.
9. Agarwal A. Gass' Atlas of Macular Diseases. 5th ed. Vol. 1. Collingwood: Saunders, 2011:4.
10. Foos RY, Simons KB. Vitreous in lattice degeneration of retina. Ophthalmology 1984;91:452-7.
11. Savige J, Liu J, DeBuc DC, et al. Retinal basement membrane abnormalities and the retinopathy of Alport syndrome. Invest Ophthalmol Vis Sci 2010;51:1621-7.
12. Gubler M, Levy M, Broyer M, et al. Alport's syndrome. A report of 58 cases and a review of the literature. Am J Med 1981;70:493-505.
13. Barker DF, Hostikka SL, Zhou J, et al. Identifi cation of mutations in the COL4A5 collagen gene in Alport syndrome. Science 1990;248:1224-7.
14. Mochizuki T, Lemmink HH, Mariyama M, et al. Identifi cation of mutations in the alpha 3(IV) and alpha 4(IV) collagen genes in autosomal recessive Alport syndrome. Nat Genet 1994;8:77-81.
15. Yoshioka K, Hino S, Takemura T, et al. Type IV collagen alpha 5 chain. Normal distribution and abnormalities in X-linked Alport syndrome revealed by monoclonal antibody. Am J Pathol 1994;144:986-96.
16. Rumpelt HJ, Langer KH, Schärer K, et al. Split and extremely thin glomerular basement membranes in hereditary nephropathy (Alport's syndrome). Virchows Arch A Pathol Anat Histol 1974;364:225-33.
17. Rumpelt HJ, Langer KH, Schärer K, et al. Split and extremely thin glomerular basement membranes in hereditary nephropathy (Alport's syndrome). Virchows Arch A Pathol Anat Histol 1974;364:225-33.
18. Arnold W. Considerations on the pathogenesis of the cochleo-renal syndrome (author's transl). Acta Otolaryngol 1980;89:330-41.
19. Mete UO, Karaaslan C, Ozbilgin MK, et al. Alport's syndrome with bilateral macular hole. Acta Ophthalmol Scand 1996;74:77-80.
20. Rahman W, Banerjee S. Giant macular hole in Alport syndrome. Can J Ophthalmol 2007;42:314-5.
21. Shah SN, Weinberg DV. Giant macular hole in Alport syndrome. Ophthalmic Genet 2010;31:94-7.
22. Sakarya Y, Sakarya R, Kara S, et al. Giant macular hole in Alport syndrome. Ophthalmic Genet 2011;32:64.
23. Mercé E, Korobelnik JF, Delyfer MN, et al. A new case of giant macular hole in a patient with Alport syndrome. J Fr Ophtalmol 2012;35:573-9.
24. Smiddy WE, Flynn HW Jr. Pathogenesis of macular holes and therapeutic implications. Am J Ophthalmol 2004;137:525-37.
25. Meguro A, Ideta H, Ota M, et al. Common variants in the COL4A4 gene confer susceptibility to lattice degeneration of the retina. PLoS One 2012;7:e39300.
26. Ivastinovic D, Schwab C, Borkenstein A, et al. Evolution of early changes at the vitreoretinal interface after cataract surgery determined by optical coherence tomography and ultrasonography. Am J Ophthalmol 2012;153:705-9.
相关文章
Zanmei Hua;Qiuyun Fang;Xiangyin Sha;Ruiming Yang;Zuopeng Hong,Role of Retinal Nerve Fiber Layer Thickness and Optic Disk Measurement by OCT on Early Diagnosis of Glaucoma丘蔚晴;张夏茵;赵兰琴;刘冬;温静怡;陈霞;王倩;李慧群;陈彦茹;韩彤;叶增纯;吴倩妮;林铎儒;肖辉;彭晖;林浩添,Retinal neurovascular characteristics for the diagnosis and staging of nondiabetic chronic kidney disease: a diagnostic study彭善珍;文小凤;魏来,The gut-eye axis in retinal degeneration