Unilateral focal lesions in the macula as an early presentation of syphilis
阅读量:1163
DOI:doi: 10.3978/ j.issn.1000-4432.2017.01.08
发布日期:2024-12-28
作者:
Qing Guo ,Tianxing Liu ,Dongfang Yin
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Macula
syphilis
fluorescein fundus angiography
indocyanine green angiography
chorioretinitis
posterior uveitis
摘要
A 55-year-old male complained of right eye blurry vision for 3 days. His best-corrected visual
acuity (BCVA) was 0.2 for the right eye and 1.0 for the left eye. Anterior segment and vitreous body
examinations of both eyes were normal. Yellowish-white focal lesions in the macula of the right eye were
observed and subtly changes of lesions were found along the superotemporal and inferotemporal arcades in
the macula two days later. Fluorescein fundus angiography (FFA) revealed slight ffuorescent leakage from the
lesions in the macula of the right eye, and segmental venous leakage and optic disc hyperffuorescence were
observed in both eyes. Indocyanine green angiography (ICGA) demonstrated that the lesions in the macula
of the right eye had hypofluorescence at a late stage and spectral domain optical coherence tomography
(SD-OCT) imaging of the macula showed focal impairment of the inner segment and outer segment
(IS/OS). The blood investigation indicated a positive treponema pallidum hemagglutination assay (TPPA)
and a rapid plasma reagin test (RPR) of 1:32. After antisyphilitica treatment for 6 weeks, the yellowish-white
lesions had vanished and the BCVA was 1.2 followed by restoration of the IS/OS for the right eye, with an
RPR of 1:4. In conclusion, ophthalmologists should alert unilateral focal lesions in the macula may be the
ffrst sign of syphilis. Prompt treatment is highly effective in resolving vision.
全文
Introduction
Syphilis is a bacterial infection caused by the spirochete
Treponema pallidum(1). The first signs and symptoms
of syphilis may be ocular, which can occur at any stage of
syphilis (2). Manifestations of ocular syphilis can include
interstitial keratitis; posterior uveitis; retinal vasculitis;
chorioretinitis; and retinitis (3,4). Chorioretinitis is a
common clinical presentation of syphilis and a cause of
painless severe vision loss (5,6). Acute syphilitic posterior
placoid chorioretinitis (ASPPC) characterized by large,
yellow-white geographic lesions involving the macula is
considered to be a distinct clinical presentation of ocular
syphilis (7-9). However, focal lesions in the macula usually
lead to a diagnostic challenge. Herein, we reported a case
of unilateral focal lesions in the macula in a patient who
presented with clinical and laboratory findings consistent
with a diagnosis of syphilis.
In this case, ICGA demonstrated that the lesions of the macula had significant hypofluorescence at a late stage. Some authors postulated that hypofluorescence resulted from deposition of degraded material from the RPE and photoreceptor segments (14). We considered the hypofluorescence may be because of inflammation infiltration, or choroid capillary blockage or both effects. ICGA could be used to investigate lesions and supply information for diagnosis. According to SD-OCT imaging, we observed the impairment of IS/OS without thickening and hyperreflective nodularity of RPE in the area corresponding to the fundus lesion , which were not consistent with the findings of ASPPC (8). OCT can provide more information about the pathophysiology of the disease. For this patient, vision improved to 1.2 after treatment followed by restoration of the IS/OS. So OCT could be a noninvasive method for follow-up.
In conclusion, unilateral focal lesions in the macula may be the ffrst sign of syghilis. Physicians should be aware that syphilis serology should be routinely done in every case of uveitis that requires investigation. A correct diagnosis is important to prompt treatment. Prompt treatment can result in good visual recovery for syphilis and can prevent potential irreversible complications.
Case presentation
A 55-year-old male presented with acute painless unilateral
blurred vision for 3 days without discharge, photophobia
and photopsia. The patient was generally healthy and had no
chronic medical conditions. There was no previous history
of eye diseases, trauma and surgery. The best-corrected
visual acuity (BCVA) was 0.2 for the right eye and 1.0 for
the left eye. Intraocular pressure was 16 mmHg in both
eyes. The corneas were clear and the pupils were equally round in both eyes. The anterior segment of both eyes
was normal without evidence of relative afferent papillary
defect in either eye. There were no inflammatory cells in
the vitreous of both eyes. In the macula, yellowish-white
focal lesions of the right eye were observed (Figure 1A).
Two days later, subtly changes of lesions were found
along the superotemporal and inferotemporal arcades
in the macula (Figure 1B) and BCVA was 0.12, while
the posterior of the left eye was normal. Fluorescein
fundus angiography (FFA) demonstrated (Figure 1)
slight fluorescent leakage in the macula of the right
eye, and segmen tal venous leakage and optic disc
hyperffuorescence were observed in both eyes (Figure 1D).
Indocyanine green angiography (ICGA) indicated that
the lesions in the macula of the right eye had spotty
hypofluorescence at early stage and the hypofluorescence was signiffcant at late stage (Figure 1E,F). Spectral domain
optical coherence tomography (SD-OCT) imaging of the
macula for the right eye showed focal impairment of the
inner segment and outer segment (IS/OS) (Figure 2A), while
OCT imaging of the macula for the left eye was normal.
Systemic general examination and the peripheral blood showed normal. Chest X-ray and MRI of the brain were normal. Laboratory examinations showed human immunodeffciency virus (HIV) antibodies, cytomegalovirus IgM, toxoplasma IgM antibodies, and herpes simplex virus IgM antibodies were negative. C-reactive protein (CRP) and erythrocyte sedimentation rate were normal. All other autoimmune screening tests were negative. Serum glucose level was 5.9 mmol. The blood investigation indicated the peripheral blood a positive treponema pallidum hemagglutination assay (TPPA) and a rapid plasma reagin test (RPR) of 1:32. Lumbar puncture was recommended to evaluate for CSF antibodies, but the patient declined this invasive test. After the diagnosis was confirmed to be ocular syphilis, the patient was recommended a treatment of benzathine penicillin intramuscular injection of 120 million units bilaterally once a week. Two weeks after initial treatment, visual improvement to 0.2, while OCT changes persisted in right eye (Figure 2B). After anti syphilitic treatment for 6 weeks, the yellowish-white lesions had vanished (Figure 1C) and the BCVA was 1.2 followed by restoration of the IS/OS for the right eye (Figure 2C), with an RPR of 1:4.
Focal lesions in the macula usually give rise to a diagnostic
difficulty. In up to 40% of reported cases, posterior uveitis
(choroiditis, retinitis, chorioretinitis, retina vasculitis) is more
commonly associated with an infectious cause with pathogens
that include syphilis, toxoplasmosis, and cytomegalovirus (13).
Other differential diagnoses include central serous
retinopathy, viral retinitis, and punctate inner choroidopathy.
For this case, according to clinical and laboratory findings,
the macular lesions of syphilis could be confirmed. The
macular was easy to be affected that was probably because of
the redundant circulation of macular. Systemic general examination and the peripheral blood showed normal. Chest X-ray and MRI of the brain were normal. Laboratory examinations showed human immunodeffciency virus (HIV) antibodies, cytomegalovirus IgM, toxoplasma IgM antibodies, and herpes simplex virus IgM antibodies were negative. C-reactive protein (CRP) and erythrocyte sedimentation rate were normal. All other autoimmune screening tests were negative. Serum glucose level was 5.9 mmol. The blood investigation indicated the peripheral blood a positive treponema pallidum hemagglutination assay (TPPA) and a rapid plasma reagin test (RPR) of 1:32. Lumbar puncture was recommended to evaluate for CSF antibodies, but the patient declined this invasive test. After the diagnosis was confirmed to be ocular syphilis, the patient was recommended a treatment of benzathine penicillin intramuscular injection of 120 million units bilaterally once a week. Two weeks after initial treatment, visual improvement to 0.2, while OCT changes persisted in right eye (Figure 2B). After anti syphilitic treatment for 6 weeks, the yellowish-white lesions had vanished (Figure 1C) and the BCVA was 1.2 followed by restoration of the IS/OS for the right eye (Figure 2C), with an RPR of 1:4.
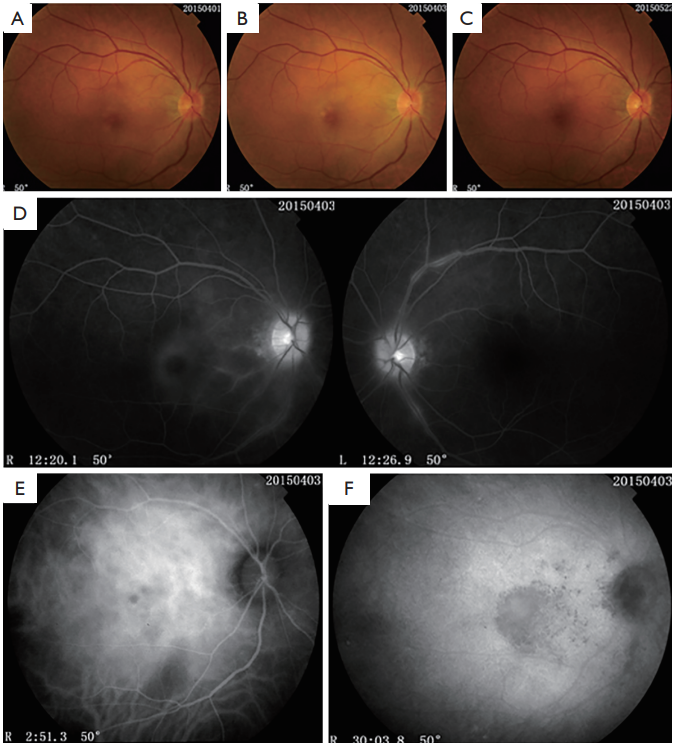
Figure 1 Eye examinations of the patient
(A) Fundus color photograph showed yellowish-white focal lesions of the right eye in the macula
at presentation; (B) showed subtly changes along the superotemporal and inferotemporal arcades in the macula two days after presentation;
(C) showed lesions vanished after treatment; (D) fluorescein fundus angiography (FFA) demonstrated slight fluorescent leakage in the
macula of the right eye, and segmental venous leakage and optic disc hyperfluorescence were observed for both eyes; (E) indocyanine
green angiography (ICGA) indicated that the lesions in the macula of the right eye had spotty hypofluorescence at early stage; (F) the
hypoffuorescence was signiffcant at late stage .
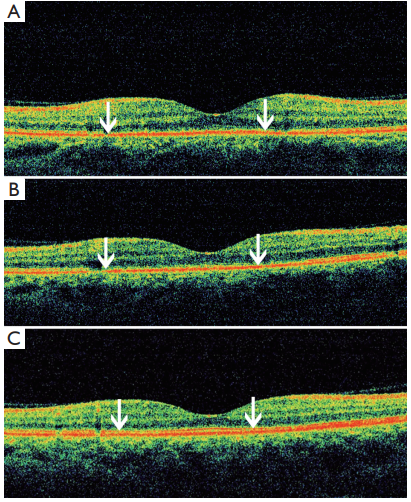
Figure 2 Spectral domain optical coherence tomography
(SD-OCT) for the case
(A) The impairment (white arrows) of the
inner segment and outer segment (IS/OS) before treatment; (B)
the impairment (white arrows) of the IS/OS persisted two weeks
after treatment; (C) restoration (white arrows) of the IS/OS six
weeks after treatment.
Discussion
The ocular presentation of syphilis is proved to be very
different among affected patients, which makes the diagnose
more challenging. There are certain features considered
to be characteristic of syphilitic uveitis. Ground glass
retinal opacification associated with retinal vasculitis is
considered to be characteristic for syphilitic uveitis (2) and
another distinctive feature is ASPPC characterized by large,
yellow-white geographic lesions involving the macula (7). In syphilitic pos terior uveitis, inflammatory changes in the
choroid, as well as in the retina, are common. Chorioretinitis
is the most common posterior segment involvement of ocular
syphilis (10). Baglivo et al. postulated that lesion of ASPPC
was focused on choroid (11). RPE impairment and vasculitis
were secondary (12). In this case, unilateral focal lesions in the
macula was ffrst found. Then, subtly changes of focal lesions
were observed along the superotemporal and inferotemporal
arcades in the macula 2 days after presentation. We also
observed the changes of retinal vasculitis and optic disc
dyeing for both eyes. It is not sure whether macular lesions of
this case was a manifestation of posterior uveitis or an early
stage of the discoid lesions. More cases need to observe to
find special features and further evolution of affecting the
macular and optic disk with syphili.
In this case, ICGA demonstrated that the lesions of the macula had significant hypofluorescence at a late stage. Some authors postulated that hypofluorescence resulted from deposition of degraded material from the RPE and photoreceptor segments (14). We considered the hypofluorescence may be because of inflammation infiltration, or choroid capillary blockage or both effects. ICGA could be used to investigate lesions and supply information for diagnosis. According to SD-OCT imaging, we observed the impairment of IS/OS without thickening and hyperreflective nodularity of RPE in the area corresponding to the fundus lesion , which were not consistent with the findings of ASPPC (8). OCT can provide more information about the pathophysiology of the disease. For this patient, vision improved to 1.2 after treatment followed by restoration of the IS/OS. So OCT could be a noninvasive method for follow-up.
In conclusion, unilateral focal lesions in the macula may be the ffrst sign of syghilis. Physicians should be aware that syphilis serology should be routinely done in every case of uveitis that requires investigation. A correct diagnosis is important to prompt treatment. Prompt treatment can result in good visual recovery for syphilis and can prevent potential irreversible complications.
基金
暂无基金信息
参考文献
1. Margo CE, Hamed LM. Ocular syphilis. Surv Ophthalmol 1992;37:203-20.
2. Benson CE, Soliman MK, Knezevic A, et al. Bilateral papillitis and unilateral focal chorioretinitis as the presenting features of syphilis. J Ophthalmic Inffamm Infect 2015;5:16.
3. Lee SB, Kim KS, Lee WK, et al. Ocular syphilis characterised by severe scleritis in a patient infected with HIV. Lancet Infect Dis 2013;13:994.
4. Bonnin N, Laurichesse H, Beytout J, et al. Ophthalmologists play a key role in the management of syphilis presenting with ocular involvement. Acta Ophthalmol 2014;92:e328-9.
5. Pan SW, Yusof NS, Hitam WH, et al. Syphilitic uveitis: report of 3 cases. Int J Ophthalmol 2010;3:361-4.
6. Yang B, Xiao J, Li X,et al. Clinical manifestations of syphilitic chorioretinitis: a retrospective study. Int J Clin Exp Med 2015;8:4647-55.
7. Gass JD, Braunstein RA, Chenoweth RG. Acute syphilitic posterior placoid chorioretinitis. Ophthalmology 1990;97:1288-97.
8. Burkholder BM, Leung TG, Ostheimer TA, et al. Spectral domain optical coherence tomography ffndings in acute syphilitic posterior placoid chorioretinitis. J Ophthalmic
Inflamm Infect 2014;4:2.
9. de Souza EC, Jalkh AE, Trempe CL, et al. Unusual central chorioretinitis as the ffrst manifestation of early secondary syphilis. Am J Ophthalmol 1988;105:271-6.
10. Samson CM, Foster CS. Syphilis. In: Foster CS, Vitale AT, editors. Diagnosis and Treatment of Uveitis. Philadelphia: WB Saunders. 2001:237-43. chap.15.
11. Baglivo E, Kapetanios A, Safran AB. Fluorescein and indocyanine green angiographic features in acute syphilitic macular placoid chorioretinitis. Can J Ophthalmol 2003;38:401-5.
12. Teplinskaia LE, Kaliberdina AF, Zaĭtseva NS, et al. Clinical-immunological disorders in uveitis in patients with Behçet's syndrome. Vestn Oftalmol 1994;110:23-5.
13. Lee MI, Lee AW, Sumsion SM, et al. Don't Forget What You Can't See: A Case of Ocular Syphilis. West J Emerg Med 2016;17:473-6.
14. Benhamou N, Souied EH, Zolf R, et al. Adult-onset foveomacular vitelliform dystrophy: a study by optical coherence tomography. Am J Ophthalmol 2003;135:362-7.
相关文章
李珑玥;杨博宇;梁凌毅,A case of interface fluid syndrome following the enhancement surgery after small incision lenticule extractionOutcomes of additional posterior to ridge diode laser versus conventional laser anterior to ridge in severe stage 3 retinopathy of prematurity—a randomized control trial林丽霞;陈苗;顾建军,Prognostic nomogram for patients with primary conjunctival malignant tumors: a study based on SEER data