Construction of databases: advances and significance in clinical research
阅读量:1247
DOI:doi: 10.3978/ j.issn.1000-4432.2015.11.13
发布日期:2024-12-30
作者:
Erping Long ,Bingjie Huang ,Liming Wang ,Xiaoyu Lin ,Haotian Lin
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Database
clinical research
data management
reanalysis of randomized controlled trials (reanalysis of RCTs)
cloud computing
摘要
Widely used in clinical research, the database is a new type of data management automation
technology and the most efficient tool for data management. In this article, we first explain some basic
concepts, such as the definition, classification, and establishment of databases. Afterward, the workflow for
establishing databases, inputting data, verifying data, and managing databases is presented. Meanwhile, by
discussing the application of databases in clinical research, we illuminate the important role of databases in
clinical research practice. Lastly, we introduce the reanalysis of randomized controlled trials (RCTs) and
cloud computing techniques, showing the most recent advancements of databases in clinical research.
全文
Introduction
Database technology, created in the 1960s, is defined
as data collection associated with special structural
organization, storage, and application in a computer
system for certain purposes, and it is the most efficient
tool for data management. Throughout the research
process, data management is critical for clinical trials. As
database technology is widely used in clinical research,
it not only makes collecting and storing the data more
convenient and reliable but also makes data analysis more
efficient, greatly improving the efficiency of research and
the rapid development of clinical studies. However, with
the development of modern science and technology, the
reanalysis of randomized controlled trials (RCTs) and
cloud computing techniques have emerged in database
applications, which have brought about not only challenges
and opportunities but also more convenience and
possibilities. Holistically grasping the important role and
the latest developments of database construction in clinical
research has become one of the most important daily tasks
for the majority of clinical researchers.
Although cloud computing, real-time databases, and intelligent analysis are high-tech areas that are still in exploratory stages, the translation and application of these new technologies to clinical research and analysis will advance clinical research models into a new era of big data.
Databases for clinical research data management, definitions and types of database, and key factors for their construction
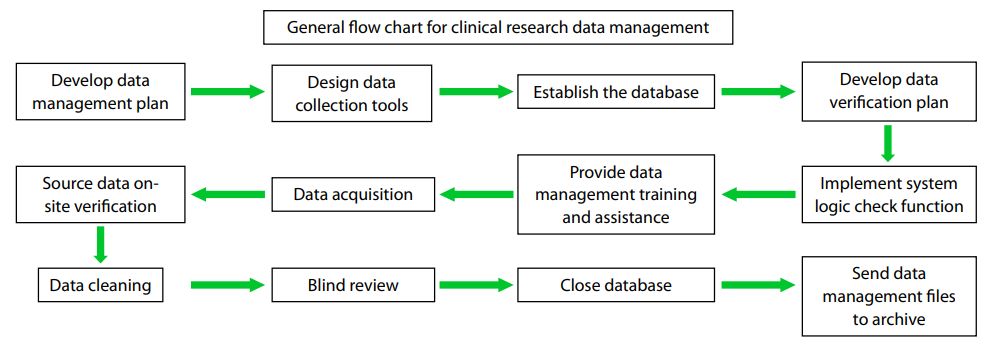
Clinical research data management includes verifying the
completeness and correctness of the data collection in
clinical trials, ensuring the support of experimental data
by statistical analyses, and illustrating and interpreting
the results of experiments, all throughout the clinical
research process. Traditionally, clinical data management
has an internationally recognized general procedure (1),
as summarized in Figure 1. Currently, clinical trial data
acquisition methods are mainly classified as one of two types, i.e., paper data capture (PDC) and electronic data
capture (EDC ). Overall, EDC has the advantages of
improving test efficiency and data quality, reducing costs,
shortening the study period, decreasing loss, and enhancing
the user’s experience; the development and application
of EDC tools in the field of clinical research have greatly
promoted the process of digitalization in clinical data
management.
Based on the complexity of the data model, database technology can be accordingly divided into three stages, i.e., the first-generation nest and hierarchical database system, the second-generation relational database system, and the third-generation database system mainly featuring object-oriented models. With the increasing data types and complexity of the data association, nested and layered databases solely relying on the tree-root node styled structure have been unable to meet the growing demand for database functions and have been mostly discarded. At present, the most popular structure is the second generation relational database, consisting of relational data structures. This type of database classifies, merges, and selects data through transforming the data structure into a two-dimension relational form and builds data platforms with complex and comprehensive management functions. However, different applications have specific functional requirements for databases that cannot be completely covered by relational databases. Therefore, the third generation databases, with richer data models and more personalized functions of management and analysis, have emerged but have only been applied to a small number of fields, such as military applications, because of the limitation of their high cost (2).
Three factors are critical to successful database construction: management, data, and technology. First, management is the foundation of database construction, which includes decisions in the early stages and the formulation of corresponding policies, strategies, and measures; software development management, data acquisition, and quality control surrounding software engineering in the development stage; the security, confidentiality, updating, and restructuring of data; and the three types of maintenance management for application software (corrective maintenance, adaptive maintenance, and improvement maintenance) in the stages of service and maintenance. Second, data are the basis of database construction, and the reliability and stability of the data source are the prerequisites for everything else associated with the database, so stricter requirements for data collection, entry, and processing have been proposed. Lastly, technology is the most direct security for database construction and has wide and complex applications, mainly including database technology, computer technology, and network and communication technologies (4).
Figure 1 General flowchart for clinical research data management.
A database is an advanced stage of data management and
distinctively different from the traditional data management
approaches mainly in the following aspects: first, databases
make the data independent of applications, thereby
enabling centralized data management and improving
the efficiency of data through data sharing and reducing
data redundancy; second, they establish links between
different databases so that the connection between real world
information is reflected; therefore, the database is no
longer just a simple tool for data collection (2). According
to its nature, a database can be divided into one of three
categories: literature databases, numerical databases, and
factual databases, each of which can be further subdivided.
Literature databases include professional literature
databases, library bibliographic databases, combined catalog
databases, patent literature databases, full-text databases,
and others. Numeric databases include scientific databases,
engineering and technology databases, and others. Factual
databases include economic and business databases,
management databases, public services databases, and
others (3). All three main categories of databases have been
widely used in clinical studies. Based on the complexity of the data model, database technology can be accordingly divided into three stages, i.e., the first-generation nest and hierarchical database system, the second-generation relational database system, and the third-generation database system mainly featuring object-oriented models. With the increasing data types and complexity of the data association, nested and layered databases solely relying on the tree-root node styled structure have been unable to meet the growing demand for database functions and have been mostly discarded. At present, the most popular structure is the second generation relational database, consisting of relational data structures. This type of database classifies, merges, and selects data through transforming the data structure into a two-dimension relational form and builds data platforms with complex and comprehensive management functions. However, different applications have specific functional requirements for databases that cannot be completely covered by relational databases. Therefore, the third generation databases, with richer data models and more personalized functions of management and analysis, have emerged but have only been applied to a small number of fields, such as military applications, because of the limitation of their high cost (2).
Three factors are critical to successful database construction: management, data, and technology. First, management is the foundation of database construction, which includes decisions in the early stages and the formulation of corresponding policies, strategies, and measures; software development management, data acquisition, and quality control surrounding software engineering in the development stage; the security, confidentiality, updating, and restructuring of data; and the three types of maintenance management for application software (corrective maintenance, adaptive maintenance, and improvement maintenance) in the stages of service and maintenance. Second, data are the basis of database construction, and the reliability and stability of the data source are the prerequisites for everything else associated with the database, so stricter requirements for data collection, entry, and processing have been proposed. Lastly, technology is the most direct security for database construction and has wide and complex applications, mainly including database technology, computer technology, and network and communication technologies (4).
Construction of clinical databases and procedures for data entry, review, and management
Database construction, data entry, review, and management
are very complex and meticulous processes, as shown in
Figure 2. However, in actual operations, attention should be
paid to the following aspects: (I) verifying the source of data,
which mainly includes data from the site of the research and
the associated laboratories. Then, the data to be collected
(i.e., the research variables), the definitions of the variables
(i.e., definitions for concept and operation), the description
of the database (i.e., the data type, single or replicate), a
confirmatory note on the consistency between the data and
the raw data, and a confirmatory note on data validation
(i.e., inspections on the values and the data range, missing
values, and logic checks) are all entered; (II) collecting and
reviewing the data, which requires timeliness, completeness,
and accuracy. Specifically, first, “timeliness” is to ensure
the quality of the raw data and to reduce the time required
for the subsequent review; “completeness” is to require
the collection of all the data on the subject; and “accuracy”
is to require that first, the designed case report should
have better operability, quantitative indicators should be
adopted as much as possible, and appropriate quantification
should also be applied to the soft indicators. Second,
the laboratory conditions and operators should be kept
relatively constant. Third, the clinicians or data collectors
who collect the data or fill out the case report forms must
be subjected to certain training. Fourth, recoding data from
the raw data should be minimized; in case of recoding,
careful reviews must be performed to ensure consistency
between the case report forms and the original data. After
completing the data collection, data review is necessary,
which includes self-review and supervision and inspection;
(III) coding, which includes manual coding and automatic
coding techniques including dictionaries (MedDRA,
WHO-ART, ICD, COSTART ); (IV) data quality control.
Commonly used methods include data tracking, data entry
and validation, data verification, data questionnaires, checks
using computer programs, and others; (V) data verification
before and after data entry. Clinical data are verified by
qualified medical inspectors; verification includes examining
and assessing complex clinical data to find subtle difference
in the data, after which data managers perform quality
control on the evaluation; ( VI) formal data entry and
database construction. The requirements for data entry
are either that problematic data should be resolved and the
entry and verification of major data should be complete
or the data have been sampled for quality control, and the
major data related to safety and effectiveness have been
evaluated with quality control checks, and all of the events
that are not in accordance with research programs have
been reported, categorized, and clarified with the related
effects. After the entry has been completed and has met
the requirements, data collation can be performed, and the
data can be transmitted to the final database; (VII) blind
data verification and database locking. After confirming the authenticity of the information and completing the blind
data verification, the database is locked, and the process
proceeds to the final analysis; the objectives and order of the
analysis are further clarified together with the researchers.
Then, the database is accepted, and a preliminary analysis
on the information is conducted, which is followed by a
preliminary data analysis to develop the draft report for
the last analysis or revised statistical analysis plan. After
verification, the database should be locked to prevent misuse
and unauthorized modification, and a list of data required
by the clinical study report should be generated. Lastly, the
data are transmitted and archived, in which the data are
sent to sponsors, statisticians, and compliance supervising
departments (5).
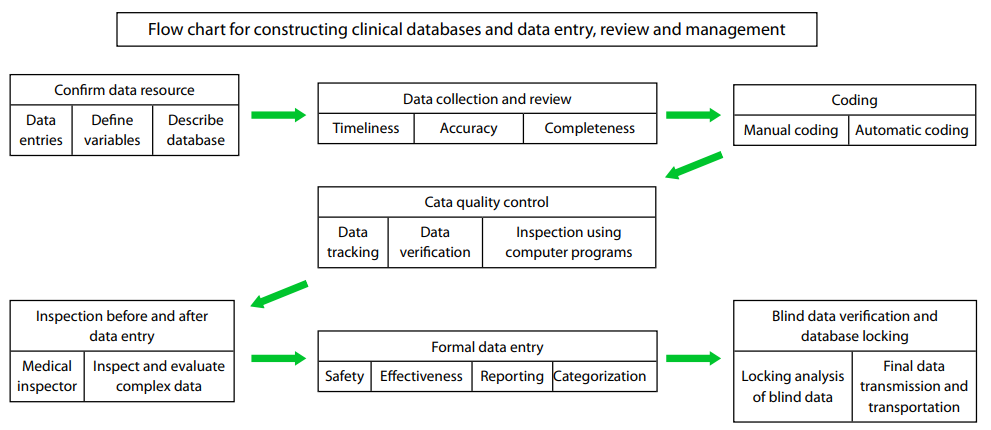
Figure 2 Flowchart for constructing clinical databases and data entry, review and management.
The important role for the clinical database on determining the level of clinical research
The important role for the clinical database on determining
the level of clinical research is mainly reflected in the
following aspects: first, a clinical database is a prerequisite
for data analysis and reaching a conclusion; second, a clinical
database is one of the measurement bases for the level of
research. The huge amount of data generated in a clinical
study can greatly improve both the efficiency of research
and the value of data through regularizing the database, and
it can provide lessons and bases for researchers in the long term
process of the study. Analyzing the database can test
the clinical study and reveal significance as well as determine
the authenticity and reliability of the clinical study, thus
effectively regulating the design and implementation of the
clinical study (6). The data in clinical research are collected
and managed in real-time, and any data management
mistakes may break the original tightly interlocking links in
the clinical trial, resulting in a loss that cannot be reversed
afterward. The quality of the data management reflects
the implementation status of the experimental design and
scheme by the investigator in the clinical trial, while alluding
to the scientifi c approach and knowledge level of the clinical
researchers. Data management is also often subjected to the
largest part of the audit of the implementation of clinical
research and is one of the major responsibilities of supervisors
and inspectors (7).
Effect of the reanalysis of RCTs on the conclusions of a study
The reanalysis of RCTs is one of the latest developments for
databases applied to clinical research. In 2014, the Journal
of the American Medical Association published a landmark
study on the reanalysis of RCTs, in which the investigators
found that in 37 cases, only five authors who reanalyzed
RCTs were totally unrelated to the initial experiments.
In terms of the experimental method, in the 37 cases,
46 different methods, including statistics and analysis
methods, were applied, and in the RCT reanalysis results,
35% of the reanalysis drew different conclusions about
patient treatment method from the initial experiments (8).
This experiment representatively indicated that the
reanalysis of RCTs on data from existing clinical studies
is feasible and can come to either the same or different
conclusions as the original trial. The role of the reanalysis is
to examine and supplement the initial experimental results
or to find loopholes and errors. However, this analysis
method still has some risks that have sparked disputes in
academia because of its short history. First, the reanalysis of
RCTs may pose a potential safety threat to patient privacy,
resulting in the exposure of patient medical information.
Second, inappropriate mining on data sets has occurred
in the reanalysis of RCTs. Third, forged and false results
have emerged in some reanalysis of RCTs. Fourth, some
reanalysis of RCTs led to the leak of trade secrets (9).
Currently, only a limited number of reanalysis of RCTs have been reported in the literature, and the investigators of the reanalysis and the methods that were adopted all affected the results of the analysis (8,9). Therefore, at present, the quality and credibility of the reanalysis of RCTs are worrisome, and it is imperative to promulgate standards of data sharing and RCT reanalysis that are more authoritative and have a broader influence. Only after a unified and authoritative standard is developed will it be possible to mitigate various issues such as the violation of patient privacy, trade secret leaks, or experiments performed to advance a particular agenda, among others, so that RCT reanalysis can be as effective as possible.
In recent years, the application of cloud computing in databases has resulted in new advances such as data clouds, real-time data, intelligent analysis of data, and others, providing new ideas for solving the above problems. Socalled cloud computing refers to network technology that uses a computer as a carrier and the network and the Internet as bases to provide real-time services to users. This is an adhoc service, i.e., it provides what the user needs and charges service fees based on the user’s usage, which greatly improves the rate of resource sharing (11). The essence of a cloud computing-based database is a large-scale centralized joint database management system, distributed across physical structures but logically belonging to the same system. The combination of cloud computing and databases has two forms: databases running in the cloud and cloud databases (12). The development of these two forms of databases is still in its infancy; while evolving in their own ways, they also bring more possibilities to database applications.
Currently, only a limited number of reanalysis of RCTs have been reported in the literature, and the investigators of the reanalysis and the methods that were adopted all affected the results of the analysis (8,9). Therefore, at present, the quality and credibility of the reanalysis of RCTs are worrisome, and it is imperative to promulgate standards of data sharing and RCT reanalysis that are more authoritative and have a broader influence. Only after a unified and authoritative standard is developed will it be possible to mitigate various issues such as the violation of patient privacy, trade secret leaks, or experiments performed to advance a particular agenda, among others, so that RCT reanalysis can be as effective as possible.
The development modes of cloud-based clinical research databases
Origin of cloud computing
After years of development, database technology has gradually matured and is playing an important role in today’s information society. However, it has also exposed some problems with its application, mainly in two aspects. First, there is an issue with updating data. Traditional databases lack real-time and initiated updates. Because there are mostly historical data in traditional data warehouses and the data retrieving cycle generally lasts several days or even a week, it is difficult to process data in real time. Meanwhile, traditional data warehouses use Extraction Transformation Loading (ETL) and adopt periodic batch updates in which the time and data of the update are preset and unable to change as needed. Second, the application scope and field of traditional data warehouses are rather narrow (10).In recent years, the application of cloud computing in databases has resulted in new advances such as data clouds, real-time data, intelligent analysis of data, and others, providing new ideas for solving the above problems. Socalled cloud computing refers to network technology that uses a computer as a carrier and the network and the Internet as bases to provide real-time services to users. This is an adhoc service, i.e., it provides what the user needs and charges service fees based on the user’s usage, which greatly improves the rate of resource sharing (11). The essence of a cloud computing-based database is a large-scale centralized joint database management system, distributed across physical structures but logically belonging to the same system. The combination of cloud computing and databases has two forms: databases running in the cloud and cloud databases (12). The development of these two forms of databases is still in its infancy; while evolving in their own ways, they also bring more possibilities to database applications.
Data cloud
Data cloud technology is based on traditional storage and storage over the Internet, supplemented with the concept of unlimited resources, aiming to become another source of RAM and hard drive space for the global network of users that are connected at high speeds and synchronically share massive amounts of data via the Internet. Studies on the data cloud are still rather preliminary, and its applications are limited by many factors, such as cost, heterogeneity, security issues, the test of time, and others. Nevertheless, Internet storage, the prototype data cloud, has long been familiar to the public and is in wide use in many countries, presenting users with great convenience; examples include well-known internet hard drives, Chinese mobile communication, Mofile, and online storage (Dostor.Com, MediaFire, OmniDrive, etc.) (13). With the continuous development and maturation of data cloud technology, it will eventually “ease the burden” for PCs and “lose weight” for the Internet, which will make RAM and hard drive capacity expand without limits, thus bringing in an unlimited amount of shared resources, prompting the whole world to progress toward greater network connectivity.Real-time databases
Another major advance in current database applications is the establishment and application of real-time databases. Real-time databases are still essentially data warehouses, but they are different from traditional databases in the most prominent feature of being real-time, reflecting the real-time changes in data warehouses: as long as there is a new event completing and generating data, the real-time database is able to capture these new data and update themselves, and the new data are immediately available. Different from the "snapshot" feature of the traditional data warehouse, a real-time data warehouse can synchronically reflect data changes in the business system (OLTP), thus making relevant analyses and decisions in real time. In short, real-time data warehouses effectively overcome the shortcomings of the traditional data warehouse, e.g., poor performance in real time and lack of capacity to provide flexible and timely tactical decisions for businesses; therefore, real-time data warehouses have broad prospects for development (10).Intelligent analysis
The increasingly large amount of data requires more demanding data mining techniques, which has prompted the emergence of technologies in intelligent analysis (14). Widely used intelligent analysis techniques can be represented by Bayesian networks(15-17), mainly used in clinical studies with an extraordinarily large scale. Compared with conventional approaches to analysis, intelligent analysis analyzes clinical data from a complete novel perspective and has broad prospects for application. With the continuous improvement in computational performance, complex high-dimensional model algorithms represented by deep learning have gradually emerged (18). Without the need for human intervention, deep learning can automatically extract features layer-by-layer from huge amounts of data and form high-dimensional data models to simulate complex data, which has surpassed the traditional algorithms in the fields of image and voice recognition and will play a crucial role in the future field of intelligent analysis (19).Although cloud computing, real-time databases, and intelligent analysis are high-tech areas that are still in exploratory stages, the translation and application of these new technologies to clinical research and analysis will advance clinical research models into a new era of big data.
基金
1. This clinical study was supported by Fundamental Research Funds of State Key Laboratory of Ophthalmology (Grant No. 2015QN01), Young Teacher Top-Suppor t
project of Sun Yat-sen University (Grant No. 2015ykzd11), the Cultivation Projects for Young Teaching Staff of Sun Yat-sen University (Grant No. 12ykpy61) from the
Fundamental Research Funds for the Central Universities, the Pearl River Science and Technology New Star (Grant No. 2014J2200060), Project of Guangzhou City, the
Guangdong Provincial Natural Science Foundation for Distinguished Young Scholars of China (Grant No. 2014A030306030) and Youth Science and Technology Innovation Talents Funds in Special Support Plan for High Level Talents in Guangdong Province (Grant No. 2014TQ01R573), Key Research Plan for National Natural Science Foundation of China in Cultivation Project (No.91546101).
参考文献
1. Li Q, Gao R, Lu F. The general procedure of clinical research data management and its management status quo. Proceedings of 13th National Conference of Clinical Pharmacology in China, 2012:522-5.
2. Cao W, Yan J. Database Review. Technology Management Research 2006;26:235-7.
3. Zhang Z. Databases and their development. Information and Documentation Services 1996;17:36-40.
4. Xu Z. Several questions about database construction. Journal of The China Society For Scientific and Technical Information 1994;13:365-9.
5. Wang T, He H, Luo Y, et al. Studies on the construction and applications of biological databases. Biotech World 2015;9:178.
6. Bazelier MT, Eriksson I, de Vries F, et al. Data management and data analysis techniques in pharmacoepidemiological studies using a pre-planned multi-database approach: a systematic literature review. Pharmacoepidemiol Drug Saf 2015;24:897-905.
7. de Waure C, Poscia A, Virdis A, et al. Study population, questionnaire, data management and sample description. Ann Ist Super Sanita 2015;51:96-8.
8. Ebrahim S, Sohani ZN, Montoya L, et al. Reanalyses of randomized clinical trial data. JAMA 2014;312:1024-32.
9. Platts-Mills TF, Jones CW. Reanalyses of trial results. JAMA 2015;313:92-3.
10. Jiang Z, Huang X. Studies on real-time data warehouse technology. Computer Systems & Applications 2007;17:91-4.
11. Yao S. Analysis of the application of database technology based on cloud computing. Computer CD Software and Applications 2013;16:296-7.
12. Wang L, Xu Y. The application and realization of a cloudbaseddatabase management system in higher education. Agriculture Network Information 2011;26:58-60.
13. Kuang S, Zhou Q, Liu X, et al. Key issues in the development of data cloud technology. Computer Science 2009;36:282-4.
14. Li G, Luo H. Studies on intelligent data analysis technology under big data. Technology Information, 2013;11:11-2.
15. Loh PR, Tucker G, Bulik-Sullivan BK, et al. Effi cient Bayesian mixed-model analysis increases association power in large cohorts. Nat Genet 2015;47:284-90.
16. Hampson LV, Whitehead J, Eleftheriou D, et al. Bayesian methods for the design and interpretation of clinical trials in very rare diseases. Stat Med 2014;33:4186-201.
17. Carreras G, Gorini G. Time trends of Italian former smokers 1980-2009 and 2010-2030 projections using a Bayesian age period cohort model. Int J Environ Res Public Health 2013;11:1-12.
18. Hinton GE, Salakhutdinov RR. Reducing the dimensionality of data with neural networks. Science 2006;313:504-7.
19. Mnih V, Kavukcuoglu K, Silver D, et al. Human-level control through deep reinforcement learning. Nature 2015;518:529-33.
相关文章
沈鸿梓;张睿峰;许梓浩;郭貔;曾婷;谭欣;艾戈晗;黄梓敬;王耿;邱坤良;彭智培;张铭志;王泓熹,Mislabeling of study designs in three Chinese general ophthalmology journals from 2021 To 2023罗明杰;张玮星;张哲铭;庞健宇;林桢哲;赵兰琴;林铎儒;林浩添,Harnessing AI–human synergy for deep learning research analysis in ophthalmology with large language models assisting humans孟丽慧;于仟仪;杨景元;陈有信,Application of anterior scleral thickness measurement in different ocular conditions using anterior segment optical coherence tomography: a systemic review