Corneal limbal stem cells are located at the limbus, the germinal center of the corneal epithelium, and are responsible for the regeneration of corneal epithelial cells by differentiation and migration to the center and surface of the cornea. Severe ocular surface diseases such as ocular chemical injuries and Steven-Johnson syndrome can result in limbal stem cell deficiency (LSCD) ,which leads to irreversible blindness by causing persistent epithelial defects, melting, perforation, conjunctivalization and vascularization of the corneal. Currently, the primary treatment of LSCD is allogeneic corneal limbal stem cell transplantation, which, however, is limited by the availability of donors and a high rejection rate. Therefore, alternative seeding cells to corneal limbal stem cells are now actively being sought in many clinical and basic studies.
Recent reports have indicated that the oral mucosal epithelium is non-keratinized and contains oral mucosal epithelial stem cells2, making it a potential substitute for limbal stem cells in the treatment of LSCD. Several studies have described clinical treatment of LSCD with autologous oral mucosal transplantation3, and reported successful reepithelialization of the corneas with LSCD following this treatment. Nonetheless, the reconstructed epithelium differed from normal corneal epithelium as it was translucent. The properties and differentiatian oif these cells, as well as their influence upon the composition of tear film, are also unknown. These are all important questions that need to be answered for the adoption of autologous oral mucosal transplantation as a treatment for LSCD. Establishing inexpensive and effective animal models will be helpful for investigating these questions and providing more precise evidence to establish the theoretical and practical basis underlying this therapy.
Here we report an animal model of for LSCD treatment by corneal autologous oral mucosal transplantation, which was established in SD rats by inducing alkali injuries to the corneal limbus followed by transplantation of autologous oral mucosal epithelium.
Materials and methods
Animals and anesthesia
Fourteen healthy SD rats, weighing 180-200g, were purchased from Guangdong Medical Laboratory Animal Center (production permit for experimental animals: SCxk(粤)2008-0002). Animals with ocular or systemic diseases were excluded. The rats were anesthetized by abdominal injection of chloral hydrate (350mg/kg). Animals were randomly assigned to Group A (autologous oral mucosal transplantation, n=7) and Group B (control, n=7) with only the right eyes being treated. The maintenance and management of experimental animals complied with the ARVO Statement for the Use of Animals in ophthalmic and Vision Research.
Equipment and reagents
Surgical microscope(TOPCON), slit-lamp camera(TOPCON), microsurgical instruments, corneal trephines with 8mm and 4mm diameters, 10-0 silk thread, 1 ml syringe, pH indicator strips, 10% chloral hydrate solution, medical povidone iodine, anhydrous ethanol, 1 mol/L NaOH, tetracaine hydrochloride eye drops, lidocaine hydrochloride solution (5ml: 0.1g), adrenalin injection, gentamicin sulfate injection(2ml: 80000U), PBS solution, tobramycin dexamethasone eye drops and ointment, and sodium fluorescein eye drops(5ml: 50mg).
Establishment of LSCD models
The animal models with LSCD were established by referring to the methods proposed by Pan et al4.Fourteen rats were subjected to intraperitoneal injection of chloral hydrate (350mg/kg) and topical anesthesia with tetracaine hydrochloride eye drops three times at 5 min intervals. The eyes and surrounding areas were prepared using medical pvoidone iodine after the disappearance of corneal reflex and covered with sterile fenestrated sheets. The surgeries were performed under an ophthalmic microscope. The whole layer of the corneal epithelium was removed with a surgical blade after treatment with anhydrous ethanol. The conjunctiva was cut open along the limbus using microsurgical scissors to expose 3mm of sclera. A ring shaped filter paper (outer and inner diameters 8 and 4mm, respectively) was made with the corneal trephines. The filter paper was then soaked in 1 mol/L NaOH for 30s and placed on the corneal limbus 0f the right eye for 30s. Excess solution was removed. The conjunctival sac was irrigated with N.S. for at least 5minutes after removing the filter paper. The pH value was monitored with pH indicator strips until it reached 7. The injuries to the corneal limbus and epithelium were assessed by fluo-rescent staining under a slit-lamp microscope. Animals in group B were treated with tobramycin dexamethasone ointment in the right eyes, while those in group A underwent autologous oral mucosal epithelial transplantation.
Autologous oral mucosa epithelial transplantation
Preparation of the oral mucosal epithelial graft: a volume of 0.2ml anesthetic containing mixed lidocaine hydrochloride and phenylephrine hydrochloride was injected underneath the oral buccal mucosa. A piece of buccal mucosa epithelium 9mm×3mm in size was cut off with microsurgical scissors and trimmed under the microscope to remove the connec- tive tissues. The submucosal connective tissues were excised as much as possible. The graft was then soaked in PBS solution containing 2000μg/ml gentamicin for 10 min. The wound in the oral mucosa was treated with iodophor solution.
The grafts were transplanted to the right eyes of the animals covering half of the corneal limbus from 12 to 60, clock. Each of the grafts was fixed to the corneal limbus by 8 stitches with 10-0 nylon sutures. Tobramycin dexamethasone ointment was applied after the procedure.
Postoperative management
Following the surgery, the treated eyes were treated with tobramycin dexamethasone eye drops 4 times daily. The following indexes were assessed and recorded under a slit-lamp microscope, including fluorescent staining area, corneal thickness, corneal transparency, neovascularization, survival of implants, ocular complications, and the condition of the oral mucosal wounds.
Results
Establishment of the LSCD model
No epithelial proliferation was observed in any of the subJects in the control group at postoperative day 14. All the corneas appeared edematous and the irises were invisible. Corneal melting occurred in 2 eyes at postoperative days 4 and 7, which proceeded to corneal perforation at postoperative days 8 and 13, respectively. The remaining five eyes showed corneal opacity and conJunctivalization.
Corneal epithelial cell healing after autologous oral mucosal epithelial transplantation
Total corneal epithelial cell defects and corneal edema occurred in all the eyes in the transplantation group on the day of surgery and 1 day but the irises may be seen indistinctly. Reepithelialization began in 6 out of 7 eyes at postoperative days 2 to 5 (median time day 3). The regenerated epithelium originated from the transplanted graft and extended toward the central cornea. Complete epithelial healing was observed on postoperative days 8 to 20 (median time day 11) , as shown by negative staining by sodium fluorescein(Figure 1). The corneal epithelia appeared translucent with the irises visible. The mucosal graft was exfoliated from one eye due to scratching by the animal. The epithelial cells failed to regenerate in the eye and corneal melting was noted at postoperative day 6, followed by Perforation at postoperative day 8.
Survival of the buccal mucosal graft
In 7 eyes from group A, 1 eye had an exfoliated graft and the remaining 6 were successfully transplanted. Slight signs of graft edema were noted on postoperative days 1 to 3, but this was gradually alleviated and disappeared on postoperative day 7, with the grafts appearing translucent and with clear margins (Figure 1).
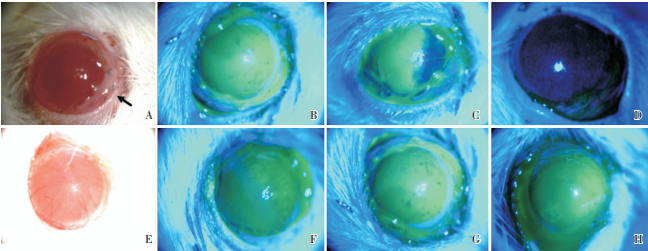
Figure 1 Postoperative slit-lamp examination of LSCD rat models transplanted autologous oral mucosa.
Figure A reveals autologous oral mucosal epithelial transplantation after establishment of LSCD models. Figure B reveals the ocular surface of LSCD models. At postoperative 1 day, a large area of fluorescent staining can be seen in both groups A (C) and B. No significant staining can be observed surrounding the buccal mucosa graft in group A (E). At 2 weeks postoperatively, dot-shaped staining of corneal epithelial cells can be noted (G). In group B, a large area of staining can be seen at both postoperative 3 days (F) and 2 weeks (H), prompting severe corneal epithelial cell defects. (Black arrow: the site of autologous oral mucosa epithelial transplantation, ×25 magnification)
Ocular complications and oral mucosal wound healing
No infectious complications occurred in eyes of group A, whereas l eye in the control group was observed with keratitis at postoperative day 4. The oral mucosal wounds healed completely in all ani- mals in Group A on postoperative Days 2 to 3. No infection or dietary disorders were noted.
Discussion
Foundation of treating LSCD with autologous oral mucosal transplantation
The oral mucosal and corneal epithelia are both non-keratinized and similar in their morphologies and arrangements. Oral mucosal epithelial cells express the cellular markers of epithelial stem cells and epithelial progenitor cells, such as P63, P75 and β1- integrin5. In addition, oral mucosal tissues are easily obtainable and the wound usually heals rapidly. These features suggest a potential role for oral mucosal epithelial cells as a substitute for corneal limbal stem cells. Most recent studies have focused on the tissue engineering of oral mucosal epithelial cells. A variety of vectors(amnion, collagen, temperature-sensitive etc.) and culture media were tested in the in vitro culture and amplification of oral mucosal epithelial cells. The engineered epithelial-cell sheets were then transplanted to the corneal surface(cultivated oral mucosa epithelial transplantation, COMET). Clinical observations of COMET in the literature, with relatively small sample sizes, have reported encouraging outcomes in early and medium terms, showing the reconstruction of corneal epithelium with COMET followed by successful phase II optical corneal transplantation. Improved ocular surface stability, corneal transparency, and visual acuity were also reported in patients receiving this therapy6,7.
To circumvent the complexity of the cell culture procedure, some researchers have also attempted autologous oral mucosal transplantation. A small-sized study3 yielded a short-term clinical outcome similar to that of COMET showing the corneas being covered by a layer of semitransparent cells. Generally, many important and unresolved problems remain for both COMET and oral mucosal transplantation, including the fate of the stem cells after transplantation, their biological behaviors, and the influences of surviving implants on the surrounding tissues and the tear film. Successful establishment of LSCD animal models treated with autologous oral mucosa transplantation will be a helpful approach to resolve these problems.
An LSCD animal model treated with autologous oral mucosal transplantation
The model of LSCD in SD rats by injuring the corneas with the sodium hydroxide solution. Successful establishment of the model was verified through nonhealing corneal epithelium, corneal melting, vascularization, and conjunctivalization. Based on these features, we transplanted an autologous oral mucosal graft onto the corneal limbus of each of the LSCD rats and confirmed that corneal reepithelialization started at 2 to 5 days postoperatively and was completed at approximately 1 to 3 weeks after transplantation. Noticeably, the epithelialization process firstly started from the directions of the oral mucosal graft, suggesting that the corneal epithelial cells most likely originated from the transplants. Finally, the corneal epithelial cells appeared to be translucent. Whether the cells originated from the oal mucosa, conjunctiva, both, or other sources, remains to be elucidated.
Key points in the model establishment
Our selection of SD rats for the model was based on the homology between rats and humans in their MHC antigens, as well as the relative simplicity of the transplantation procedure in rats compared with that in mice. Proficient microsurgical skills are re- quird to manage the rat cornea, which has a diameter of 6 millimeters. We thoroughly destroyed the corneal limbal stem cells by application of the ring- shaped filter paper with an outer diameter of 8mm and inner diameter of 4mm , which ensured that the whole limbus and peripheral cornea was covered and the injured area was sufficiently large. The filter paper should be placed for at least 30s, followed by complete irrigation with N.S. until the pH in the conjunctival sac reached 7 to avoid any negative effects on the implanted oral mucosal cells due to the alkaline environment.
Buccal mucosa belongs to the covering mucosa of the oral cavity. The mucosal epithelium is nonkeratinized, with insignificant intercellular bridge in the stratum spinosum, mobilizable, and a thin lamina propria. Submucosal injection of a mixture of lidocaine hydrochloride and phenylephrine hydrochloride could anesthetize the mucosa, separate it from the underlying connective tissues, and prevent potential hemorrhage, thus helping to obtain a thin graft with a relatively small wound. During the procedure, the bevel of the needle should be kept upwards and inserted just beneath the buccal mucosa to obtain a thin epithelial sheet with the undersurface clear. Manual sampling may result in oral mucosal sheets containing connective tissues. Any connective tissue that may have been included during the manual procedure should be removed completely from the graft under a surgical microscope before transplantation.
Compared with common experimental animals like rabbits, the corneas of rats are thinner and softer that require good microsurgical skills for management. Corneal perforations can commonly occur when implanting the oral mucosal graft, but can be prevented with 10-0 nylon sutures and proficient suturing techniques. In cases of perforation, the wound should be sutured immediately and the graft should be moved to another site.
To summarize, our study established a successful model of LSCD treated with autologous oral mucosal transplantation, which should facilitate further inquiries into the underlying biological mechanisms. Our future investigations involve elucidating the source of regenerated epithelium after transplantation, the fate and biological behaviors of the implanted stem cells, and the structural and functional influences of the graft on the tear film. We are also evaluating the efficacy of autologous oral mucosal transplantation in the treatment of LSCD by comparing it with allogeneic corneal limbal transplantation and cultivated oral mucosa epithelial transplantation.
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)