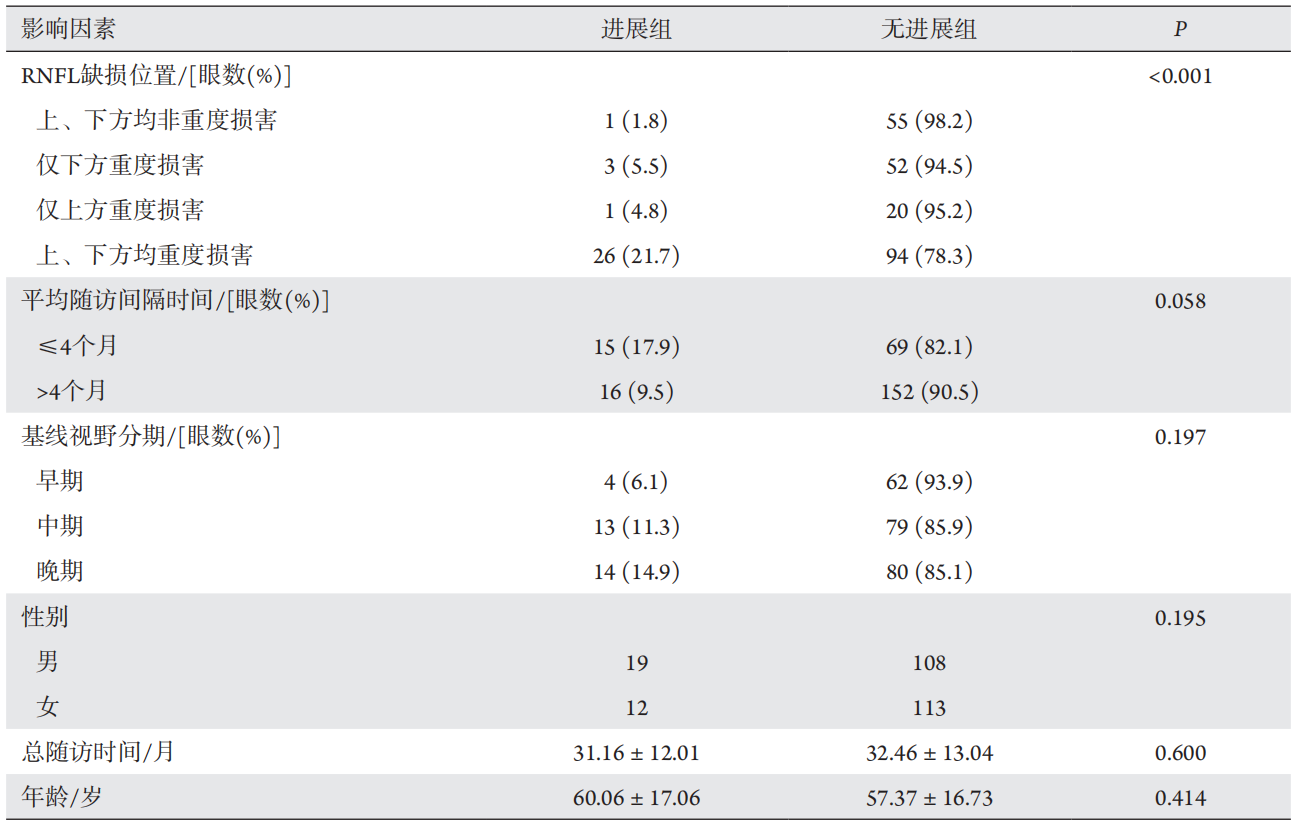
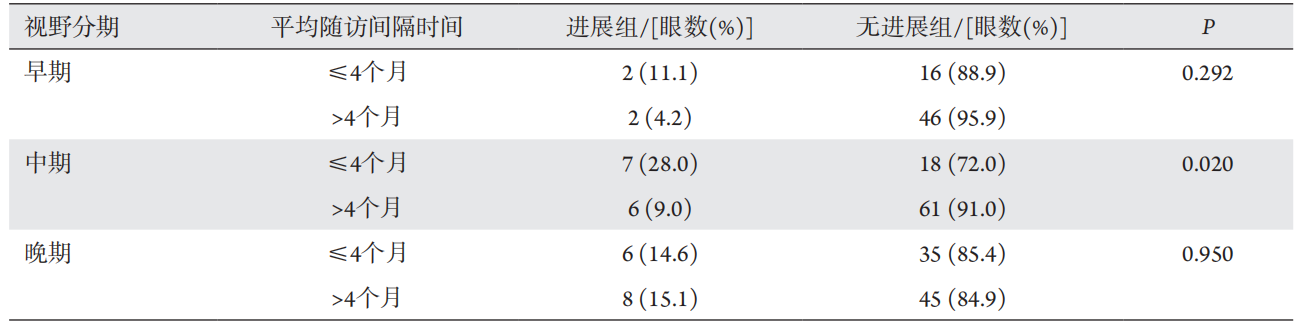
目的:了解原发性开角型青光眼(primary open angle glaucoma,POAG)患者视野缺损的进展情况,探讨其发生进展的相关危险因素。方法:回顾性分析2014年1月至2018年7月就诊于北京大学第三医院眼科并有至少4次视野检查的POAG患者。按照患者首次视野检查的平均偏差或平均缺损进行分期。将历次随访视野检查的平均偏差或平均缺损与时间进行线性回归分析,取其斜率(dB/年)。根据平均偏差或平均缺损的斜率将患者分为进展组与无进展组。分析患者视盘周围视网膜神经纤维层(retinal nerve fiber layer,RNFL)厚度损害位置、平均随诊间隔时间、基线视野分期等因素与青光眼视野缺损进展的关系。结果:共纳入128例患者(252只眼),其中129眼使用Octopus视野计检查随访,基线视野缺损值为(10.91±5.76) dB;123眼使用Humphrey视野计,基线视野偏差值为(–10.62±6.89) dB。视野缺损早、中、晚期的比例分别为26.19%、36.51%和37.30%。进展组31只眼(12.30%),无进展组221只眼(87.70%)。上下方RNFL都存在重度损害的患者,其视野缺损更易进展(P<0.001)。平均随诊间隔时间≤4个月的患眼,发生进展的比例高于平均随诊间隔时间>4个月的患眼(P=0.058)。基线视野分期、年龄、性别、总随访时间与视野缺损进展未见显著相关性。结论:青光眼患者的视功能损害出现恶化是普遍存在的。上下方RNFL均存在重度损害、随诊间隔时间短与视野缺损进展相关。视神经结构的改变与功能损害具有相关性,结构改变的方位对功能损害进展有提示功能。规律随诊对病情监测有重要意义,对于可能快速进展的患者,应缩短随诊间隔时间。
全文
青光眼是全球首位不可逆性致盲性眼病,原发性开角型青光眼(primary open angle glaucoma,POAG)是其中的重要类型。POAG以特征性的视神经结构和功能改变伴房角开放为特征,即视盘沿变窄、神经纤维层丢失与视野缺损[1-4]。POAG的治疗以降眼压为主[5-6],通过将眼压降至目标眼压范围可使大部分POAG患者病情得到有效控制,但仍有部分患者视野缺损持续进展[7]。既往研究[8-10]显示:较高的基线眼压、高龄、女性等因素可能与POAG患者视野缺损进展有关,但仍不能解释所有患者病情进展的原因。
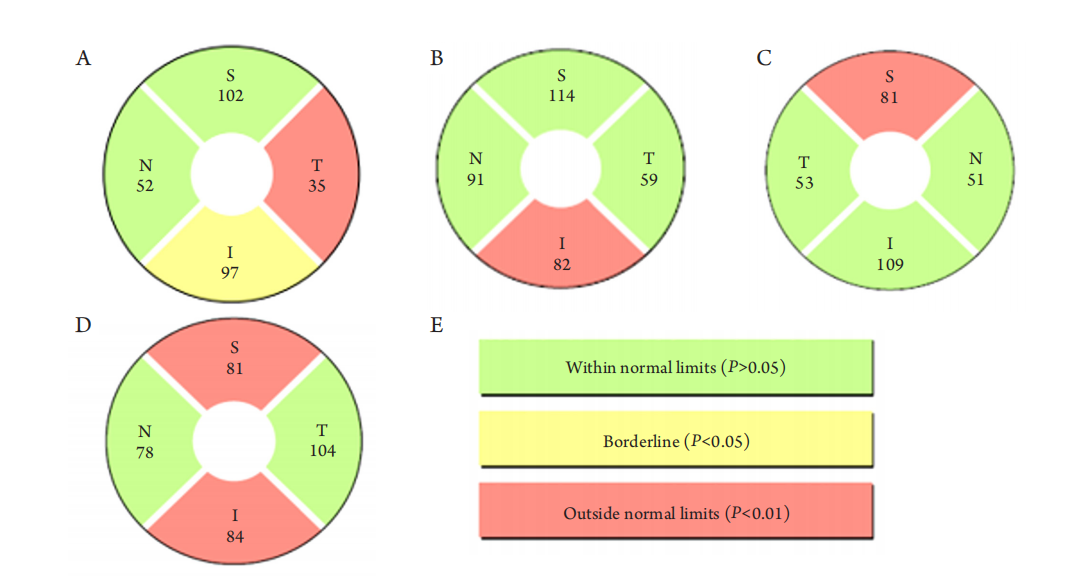
(A) Upper and lower parts of the group with non-severe damage; (B) Only the lower part of the severely damaged group; (C) Only the upper part of the severely damaged group; (D) Both upper and lower parts of the severely damaged group; (E) Meaning of OCT inspection report color.
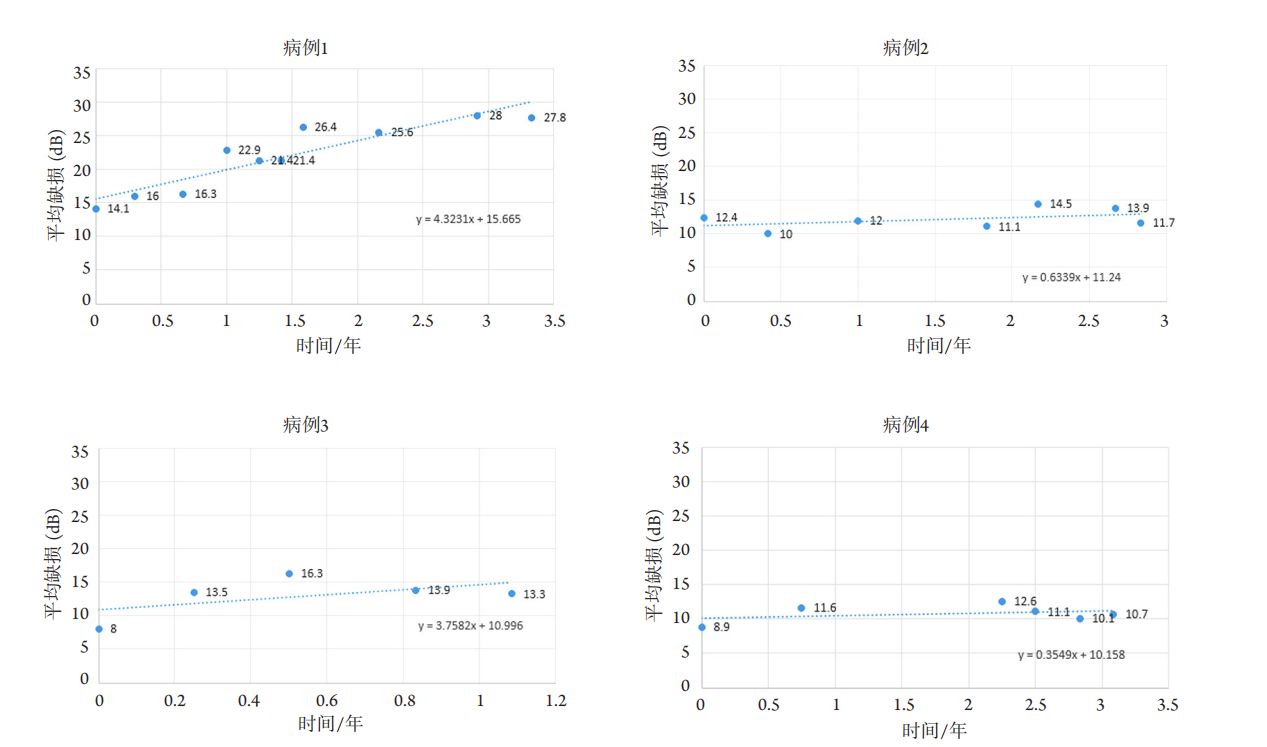
The figure shows the mean defect value of the visual field examination with the Octopus field analyzer of the patients during the previous follow-up. The slope K of the linear regression equation represents the change of the visual field defect, and K>1 represents the progress of the visual field. Case 1: patients with severe damage both above and below OCT; Case 2: patients with non-severe damage both above and below OCT; Case 3: patients with average follow-up interval ≤4 months; Case 4: average follow-up interval >4 months patient.
1. 国家自然科学基金 (81670851)。 This work was supported by the National Natural Science Foundation, China (81670851).
参考文献
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness
and distance vision impairment 1990—2020: a systematic review and
meta-analysis[ J]. Lancet Glob Health, 2017, 5(12): e1221-e1234.
2. Chan EW, Li X, Tham YC, et al. Glaucoma in Asia: regional prevalence
variations and future projections[ J]. Br J Ophthalmol, 2016, 100(1):
78-85.
3. Wu L, Sun X, Zhou X, et al. Causes and 3-year-incidence of blindness
in Jing-An District, Shanghai, China 2001-2009[ J]. BMC Ophthalmol,
2011, 11: 10.
4. 王灿, 赵平. 原发性开角型青光眼的早期诊断及研究进展[ J]. 国
际眼科杂志, 2016, 16(7): 1287-1290.
WANG C, ZHAO P. Research progress on early diagnosis of
primary open angle glaucoma[ J]. International Eye Science, 2016,
16(7): 1287-1290.
5. 王雪琼, 李军, 黎卫平. 原发性开角型青光眼的治疗现状[ J]. 临
床眼科杂志, 2017, 25(2): 183-187.
WANG XQ, LI J, LI WP. Current treatment for primary
open angle glaucoma[ J]. Journal of Clinical Ophthalmology, 2017,
25(2): 183-187.
6. The Advanced Glaucoma Inter vention Study (AGIS): 7. The
relationship between control of intraocular pressure and visual field
deterioration. The AGIS Investigators[ J]. Am J Ophthalmol, 2000,
130(4): 429-440.
7. Yokoyama Y, Maruyama K, Konno H, et al. Characteristics of patients
with primary open angle glaucoma and normal tension glaucoma at a
university hospital: a cross-sectional retrospective study[ J]. BMC Res
Notes, 2015, 8: 360.
8. Nouri-Mahdavi K, Hoffman D, Coleman AL, et al. Predictive factors
for glaucomatous visual field progression in the advanced glaucoma
intervention study[ J]. Ophthalmology, 2004, 111(9): 1627-1635.
9. Leske MC, Heijl A, Hussein M, et al. Factors for glaucoma progression
and the effect of treatment: the early manifest glaucoma trial[ J]. Arch
Ophthalmol, 2003, 121(1): 48-56.
10. Actis AG, Versino E, Brogliatti B, et al. Risk factors for primary open
angle glaucoma (POAG) progression: a study ruled in torino[ J]. Open
Ophthalmol J, 2016, 10: 129-139.
11. 游启生, 李建军. 青光眼视野损害程度的分级方法[ J]. 眼科,
2008, 17(1): 63-65.
YOU QS, LI JJ. Grading method for degree of visual field
damage in glaucoma[ J]. Ophthalmology in China, 2008, 17(1): 63-65.
12. Numata T, Matsumoto C, Okuyama S, et al. Detectability of visual field
defects in glaucoma with high-resolution perimetry[ J]. J Glaucoma,
2016, 25(10): 847-853.
13. Runji? T, Novak Lau? K, et al. Effect of different visual impairment
levels on the quality of life in glaucoma patients[ J]. Acta Clin Croat,
2018, 57(2): 243-250.
14. 张莉, 张亚琴, 张景尚, 等. 原发性开角型青光眼视神经损害进展
的相关危险因素研究:207例患者的随诊观察结果[ J]. 中华眼科
医学杂志(电子版), 2011, 1(1): 16-23
ZHANG L, ZHANG YQ, ZHANG JS, et al. Risk factors for
primary open angle glaucoma progression: follow-up of 207 cases[ J].
Chinese Journal of Ophthalmologic Medicine. Electronic Edition,
2011, 1(1): 16-23.
15. 罗毅, 祁勇军, 赵燕. 原发性开角型青光眼患者视网膜神经纤维
层厚度与视野缺损的相关性研究[ J]. 眼科新进展, 2015, 35(11):
1054-1056.
LUO Y, QI YJ, ZHAO Y. Correlation between RNFL
thickness and visual field defect in primary open-angle glaucoma
patients[ J]. Recent Advances in Ophthalmology, 2015, 35(11):
1054-1056.
16. 关新辉, 李丽, 梁勇. 应用SD-OCT纵向比较正常人群和青光眼
进展及非进展人群的RNFL厚度[ J]. 国际眼科杂志, 2016, 16(8):
1504-1507.
GUAN XH, LI L, LIANG Y. Longitudinal analysis of retinal nerve
fiber layer thickness measurement by spectral-domain optical coherence
tomography in normals and in glaucoma patients with or without
progression[ J]. International Eye Science, 2016, 16(8): 1504-1507.
17. Shin JW, Sung KR, Lee J, et al. Factors associated with visual field
progression in cirrus optical coherence tomography-guided progression
analysis: a topographic approach[ J]. J Glaucoma, 2017, 26(6): 555-560.
'%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)