Inflammatory choroidal neovascularization after tubercular posterior scleritis
阅读量:2095
DOI:doi: 10.3978/j.issn.1000-4432.2015.11.09
发布日期:2024-11-26
作者:
Remya Paulose ,Jay Chhablani
展开更多 '%20fill='white'%20fill-opacity='0.01'/%3e%3cmask%20id='mask0_3477_29692'%20style='mask-type:luminance'%20maskUnits='userSpaceOnUse'%20x='0'%20y='0'%20width='16'%20height='16'%3e%3crect%20id='&%23232;&%23146;&%23153;&%23231;&%23137;&%23136;_2'%20x='16'%20width='16'%20height='16'%20transform='rotate(90%2016%200)'%20fill='white'/%3e%3c/mask%3e%3cg%20mask='url(%23mask0_3477_29692)'%3e%3cpath%20id='&%23232;&%23183;&%23175;&%23229;&%23190;&%23132;'%20d='M14%205L8%2011L2%205'%20stroke='%23333333'%20stroke-width='1.5'%20stroke-linecap='round'%20stroke-linejoin='round'/%3e%3c/g%3e%3c/g%3e%3c/svg%3e)
关键词
Posterior scleritis
choroidal neovascular membrane (CNVM)
choroidal thickness
choroid
摘要
A 45-year-old female presented with typical features of posterior scleritis in her left eye with
visual acuity of 20/252. After treatment with oral steroids and immunosuppressive drugs, at 2 months
follow-up, posterior scleritis resolved and visual acuity improved to 20/50. Five months later she presented
with vision loss (20/160) associated with active choroidal neovascular membrane (CNVM) close to scar.
Significant choroidal thinning (subfoveal choroidal thickness =137 microns), compared to fellow eye
(subfoveal choroidal thickness =247 microns) was noted. Two doses of intravitreal bevacizumab (IVB)
were given at 1 month interval. At 9 months follow-up, her visual acuity was maintained at 20/160 with
scarred CNVM. In conclusion, IVB is safe and efficacious in treatment of inflammatory CNVM secondary
to posterior scleritis. Choroidal changes after posterior scleritis could be contributory factor for formation
of CNVM.
全文
Introduction
Posterior scleritis is a painful and under-recognized form
of scleral inflammation caused by infectious agents or
non-infectious immune reactions (1). The disease may be
associated with anterior scleritis and may spread to muscle
and other orbital tissue or the choroid and retina (2,3).
Although choroidal neovascular membrane (CNVM) in
inflammatory posterior pathology is quite well-known
and published widely (4,5), however, the same in posterior
scleritis is under reported in literature.
We herein report a case on the occurrence of inflammatory
CNVM in a patient who recovered from posterior scleritis
and was treated successfully with anti-vascular endothelial
growth factor (anti-VEGF) therapy.
Case presentation
A 45-year-old healthy female presented with complaints of
pain and reduced vision in her right eye for last 5 months
duration. On examination, best corrected visual acuity
(BCVA) was 20/252 and 20/25 in the right and left eye
respectively. Anterior segment examination was normal
in both eyes. On fundoscopy, right eye showed disc
hyperemia with blurred margins with sub retinal fluid at
the posterior pole and left eye was within normal limits.
Ultrasonography, fluroscein angiography (FA) and spectral
domain optical coherence tomography (SD-OCT) findings
confirmed the diagnosis of posterior scleritis in right eye
(Figure 1).
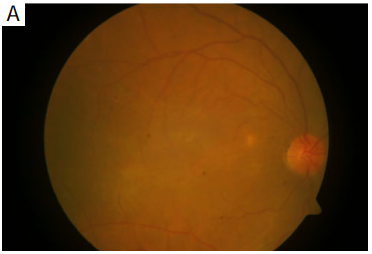
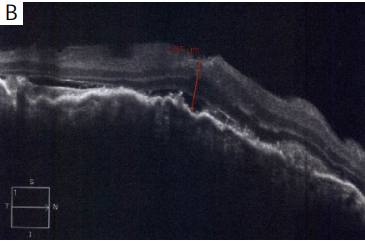
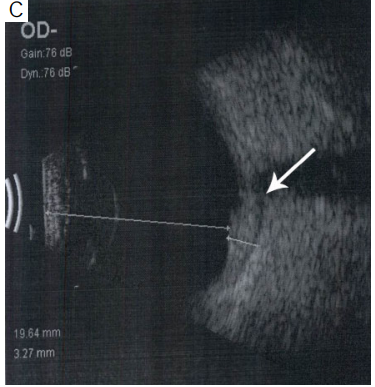
Figure 1 (A) At baseline color fundus photograph shows
hyperemic disc with retinal edema; (B) spectral domain optical
coherence tomography (SD-OCT) shows choroidal elevation with
choroidal folds along with subretinal fluid; (C) ultrasonography
shows choroidal thickening with presence of fluid (arrow) (T sign)
suggestive of posterior scleritis.
Six months later she came with further vision loss in
the same eye. On examination, visual acuity in her right
eye was 20/160. Right eye fundus showed fresh sub retinal
haemorrhages at the macula close to previously involved
area, suggestive of an active CNVM (Figure 2A). SD-OCT,
FA and indocyanine green angiography showed signs of
active choroidal neovascular membrane (Figure 2B,C,D).
After informed consent, patient underwent two injections
of intravitreal bevacizumab (IVB) (1.25 mg in 0.05 mL) at
1 month interval. One month after second injection, there
was no activity on SD-OCT; therefore, she was asked to
continue ATT as per the physician’s advice. Patient was
under regular follow-up. At 9 months follow-up after last
IVB, her BCVA was maintained at 20/160 and fundus
examination showed scarred CNVM which was confirmed
on SD-OCT (Figure 2E), along with RPE atrophy due to
recovered posterior scleritis.
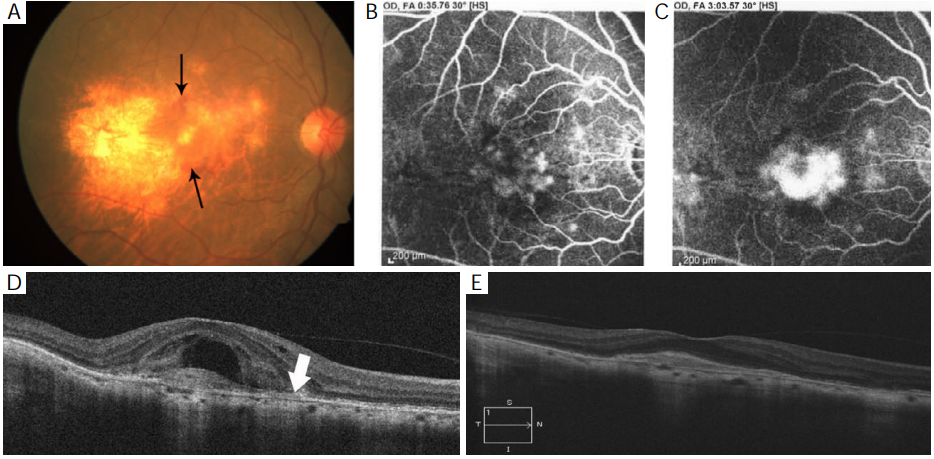 Figure 2 (A) Fundus photograph shows scarring at the macula secondary to recovered posterior scleritis along with fresh subretinal haem
(black arrow); (B,C) fundus fluorescein angiography is suggestive of active choroidal neovascularization; (D) spectral domain optical
coherence tomography (SD-OCT) showed presence of subretinal and intraretinal fluid along with choroidal neovascular membrane.
Choroidal thinning along with loss of medium sized choroidal vessels with sparing of large vessels (white arrow) also noted; (E) at 9 months
follow-up, SD-OCT scan shows no fluid with subfoveal scar.
Figure 2 (A) Fundus photograph shows scarring at the macula secondary to recovered posterior scleritis along with fresh subretinal haem
(black arrow); (B,C) fundus fluorescein angiography is suggestive of active choroidal neovascularization; (D) spectral domain optical
coherence tomography (SD-OCT) showed presence of subretinal and intraretinal fluid along with choroidal neovascular membrane.
Choroidal thinning along with loss of medium sized choroidal vessels with sparing of large vessels (white arrow) also noted; (E) at 9 months
follow-up, SD-OCT scan shows no fluid with subfoveal scar.
Discussion
Choroidal neovascular membrane formation although
uncommon is a well-known sight-threatening complication
of posterior segment intraocular inflammation. The
development of CNVM results either directly from an
inflammatory-mediated angiogenic drive and/or secondary
to a degenerative disruption in the Bruch’s membraneretinal
pigment epithelium (RPE) complex. VEGF is a key
inducer of neovascularization (6).
Uchihori et al. reported that high-penetration optical coherencetomography (HP-OCT) measurements performed in two patients with acute posterior scleritis showed thickened choroids. After treatment, the choroidal thickness decreased (7). Similarly in our patient the choroidal thickness was found to be reduced to 137 microns after the resolution of posterior scleritis compared to 247 microns in the fellow eye.
Involvement of choroid in posterior scleritis is also supported by studies conducted by Auer and Herbort (8), who reported that that posterior scleritis induces major alterations in the adjacent choroid, confirmed on indocyanine green angiography. Initial enhanced depth imaging optical coherence tomography (EDI-OCT) in our case showed minimal changes in the choriocapillaries along with increased choroidal thickness, but as the posterior scleritis resolved it was seen that in addition to the reduced choroidal thickness there was loss of medium sized choroidal vessels and choriocapillaries, sparing only larger choroidal vessels (Figure 2D,E). From this observation, we speculate that inflammation of the posterior sclera induces alterations in the adjacent choroid, gradually leading to choroidal atrophy and changes in the integrity of Bruch’s membrane finally favouring the development of a neovascular membrane.
Currently, various options are available for managing inflammatory CNVM including laser photocoagulation, local and systemic corticosteroids, and surgical removal; all with potential limitations (9,10). To date, clinical trials evaluating the treatment options for inflammatory CNVM associated with uveitis have been limited and mostly non-comparative. Successful management involves both control of intraocular inflammation and occlusion of the inflammatory neovascular membrane. Median number of anti-VEGF injections required in treatment of inflammatory CNVM has been reported to be to 1.73 (range, 1-5) (5). Similarly in our patient, two IVB injections led to CNVM regression as well as improvement and stabilization of vision with no recurence till 9 months follow-up.
Although, significant advances have recently occurred in the understanding of choroidal changes in posterior scleritis, further understanding about the vascular changes in choroid is still warranted. These significant choroidal vascular changes in various inflammatory conditions could be targeted for therapy and could be used to predict the occurrence of CNVM in future.
Uchihori et al. reported that high-penetration optical coherencetomography (HP-OCT) measurements performed in two patients with acute posterior scleritis showed thickened choroids. After treatment, the choroidal thickness decreased (7). Similarly in our patient the choroidal thickness was found to be reduced to 137 microns after the resolution of posterior scleritis compared to 247 microns in the fellow eye.
Involvement of choroid in posterior scleritis is also supported by studies conducted by Auer and Herbort (8), who reported that that posterior scleritis induces major alterations in the adjacent choroid, confirmed on indocyanine green angiography. Initial enhanced depth imaging optical coherence tomography (EDI-OCT) in our case showed minimal changes in the choriocapillaries along with increased choroidal thickness, but as the posterior scleritis resolved it was seen that in addition to the reduced choroidal thickness there was loss of medium sized choroidal vessels and choriocapillaries, sparing only larger choroidal vessels (Figure 2D,E). From this observation, we speculate that inflammation of the posterior sclera induces alterations in the adjacent choroid, gradually leading to choroidal atrophy and changes in the integrity of Bruch’s membrane finally favouring the development of a neovascular membrane.
Currently, various options are available for managing inflammatory CNVM including laser photocoagulation, local and systemic corticosteroids, and surgical removal; all with potential limitations (9,10). To date, clinical trials evaluating the treatment options for inflammatory CNVM associated with uveitis have been limited and mostly non-comparative. Successful management involves both control of intraocular inflammation and occlusion of the inflammatory neovascular membrane. Median number of anti-VEGF injections required in treatment of inflammatory CNVM has been reported to be to 1.73 (range, 1-5) (5). Similarly in our patient, two IVB injections led to CNVM regression as well as improvement and stabilization of vision with no recurence till 9 months follow-up.
Although, significant advances have recently occurred in the understanding of choroidal changes in posterior scleritis, further understanding about the vascular changes in choroid is still warranted. These significant choroidal vascular changes in various inflammatory conditions could be targeted for therapy and could be used to predict the occurrence of CNVM in future.
基金
暂无基金信息
参考文献
1. McCluskey PJ, Watson PG, Lightman S, et al. Posterior scleritis: clinical features, systemic associations, and outcome in a large series of patients. Ophthalmology .1999;106:2380-6.
2. Chavis RM, Garner A, Wright JE. Infl ammatory orbital pseudotumor. A clinicopathologic study. Arch Ophthalmol.1978;96:1817-22.
3. Rootman J, Nugent R. The classifi cation and management of acute orbital pseudotumors. Ophthalmology.1982;89:1040-8.
4. Wu L, Evans T, Saravia M, et al. Intravitreal bevacizumab for choroidal neovascularization secondary to Vogt Koyanagi-Harada syndrome. Jpn J Ophthalmol.2009;53:57-60.
5. Arevalo JF, Adan A, Berrocal MH, et al. Intravitreal bevacizumab for infl ammatory choroidal neovascularization: results from the Pan-American Collaborative Retina Study Group at 24 months. Retina. 2011;31:353-63.
6. Grossniklaus HE, Ling JX, Wallace TM, et al. Macrophage and retinal pigment epithelium expression of angiogenic cytokines in choroidal neovascularization. Mol Vis.2002;8:119-26.
7. Uchihori H, Nakai K, Ikuno Y, et al. Choroidal observations in posterior scleritis using high-penetration optical coherence tomography. Int Ophthalmol 2014;34:937-43.
8. Auer C, Herbort CP. Indocyanine green angiographic features in posterior scleritis. Am J Ophthalmol 1998;126:471-6.
9. D'Ambrosio E, Tortorella P, Iannetti L. Management of uveitis-related choroidal neovascularization: from the pathogenesis to the therapy. J Ophthalmol 2014;2014:450428.
10. O'Toole L, Tufail A, Pavesio C. Management of choroidal neovascularization in uveitis. Int Ophthalmol Clin 2005;45:157-77.
相关文章
黎雅姬;陈雪琳;马进;吉宇莹,Nanophthalmos associated with acute ischemic optic neuropathy: a case report and literature review蔡晨希;崔金利;王强;李涛;刘炳乾;林振强;熊晓媚;刘泽浩;林英,Visual prognosis of vitrectomy for polypoidal choroidal vasculopathy with breakthrough vitreous hemorrhage Chunyi Wei;Ran Liu;Jiaqing Li;Yu Yang;Xiaoyan Ding,Choroidal Analysis of Polypoidal Choroidal Vasculopathy by Spectral Domain Optical Coherence Tomography